Introduction:
Amelogenesis Imperfecta (AI) has been described as a group of hereditary conditions that disturbs the developing enamel structure and exists independent of any related systemic disorder.[1],[2] AI is caused by mutations in genes that control amelogenesis and follows inheritance patterns of autosomal-dominant, autosomal recessive or X-linked modes of transmission.[3],[4] The incidence of AI has been reported as varying between 1:700 and 1:16,000, depending on the diagnostic criteria and the population studied.[5]
Witkop and Sauk listed the verities of Amelogenesis Imperfecta, divided according to weather abnormality lay in a reduced amount of enamel (Hypoplasia), deficient calcification hypocalcification, or imperfect maturation of the enamel (hypomaturation) and also recognized the combined defects.[6]
According to Seow, the primary clinical problems of AI are esthetics, dental sensitivity and decreased occlusal vertical dimensions.[7] Restoration of these defects is important not only because of esthetic and functional concerns, but also because there may be a positive psychological impact for the patient.[1].
This clinical report describes a case of 22-year old male patient with Amelogenesis Imperfecta
Case Report:
A 22-year-old male patient was referred to the Department of Oral Pathology and Microbiology, Purvanchal Institute of Dental Sciences, Gorakhpur with the chief complaint of generalized discoloration of permanent teeth since their eruption. Patient also complains of generalized sensitivity of his teeth to both heat and cold. Past dental history reveals, there was generalised discoloration of his deciduous teeth even. Medical history was non-contributory. Patient’s family history revealed that his mother is also having similar generalized discoloration of teeth.
Clinical examination of patient showed that the enamel of all the teeth were hypoplastic and yellowish in color with occasional white flakes on anterior teeth.(Figure 1) The surfaces of the teeth were rough and the enamel covering the anterior teeth were very thin. In some of the posterior teeth, enamel was lost due to attrition with severe staining of exposed dentin.(Figure 2).
 | Figure 1 : Yellowish Discoloration With Occasional White Flakes On Anterior Teeth And Spacing In Maxillary Anterior Teeth.
 |
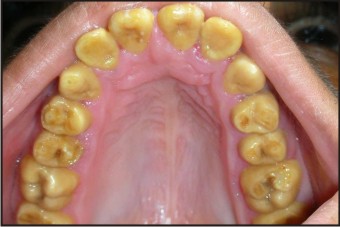 | Figure 2 : Occlusal View Showing Attrition With Exposure Of Dentin.
|
The maxillary anterior teeth show spacing. The vertical height was not lost. Vitality test was done on all teeth using electric pulp tester, and all the teeth were vital and non-tender to percussion.
Radiographic investigations included an Orthopantomogram (OPG). The OPG showed the presence of unerupted 18, 28, 38, 48. The thickness of enamel was less compare to normal and radiodensity of enamel and dentin were almost same making differentiation between the two difficult. OPG also shows wide pulp chambers in some of the posterior teeth. (Figure 3).
 | Figure 3 : Pre-operative Orthopantomogram (Opg).
|
After thorough examination, the patient was diagnosed as having hypomaturation type of AI because the thickness of enamel was normal and hard in texture but mottled, opaque white to yellow brown in color.
Esthetics was the main reason that brought him to the hospital for treatment. The treatment proposed for her ranged from restoration of decayed teeth, Extraction of impacted teeth and direct composite restoration of anterior teeth.
In the treatment plan, the restorative procedure alternatives were explained to the patient, including the differences in costs, the levels of tooth structure removal, the expected clinical longevity, the time period necessary the conclude the treatment, and the possible esthetic results. A treatment plan was developed with the aim of improving the patient's esthetic appearance with direct composite restorations.
Labial surfaces of all the teeth selected for composite restorations were reduced using a rotary flat end tapered fissure bur to about 0.5 to 0.8mm depth, so that the final tooth preparation to be confined within enamel.(Figure 4) As bonding of composite resin to enamel is much superior than to that of to dentin.
 | Figure 4 : Reduction Of Labial Surfaces For Direct Composite Restoration.
|
The teeth were conditioned and primed with a self-etching adhesive (Clearfil SE Bond, Primer; Kuraray Medical, Tokyo, Japan) for 20 seconds. Then the etchant was removed using water spray for 5 seconds. Bonding agent (Clearfil SE Bond; Kuraray Medical Inc) was then applied and polymerized for 10 seconds with a polymerizing light unit (Bluephase C5, Ivoclar, Vivadent).
The restorations were formed using a hybrid resin composite (Ecusit System, DMG, Hamburg, Germany), an incremental technique. The resin composite restorations were polymerized for at least 60 seconds per increment with the polymerization light unit (Bluephase C5, Ivoclar Vivadent). Finishing and polishing was done using sof-lex discs and shofu composite polishing kit.(Figure 5).
 | Figure 5 : After Direct Composite Resin Restorations.
|
Discussion:
Amelogenesis imperfecta (AI) encompasses a heterogeneous group of developmental disorders that demonstrate alterations in the enamel.[3] It is characterized by clinical symptoms in the absence of other systemic abnormalities or diseases.[3],[4] Amelogenesis Imperfecta is caused by mutations in genes that control formation of enamel and follows inheritance patterns of autosomal-dominant, autosomal recessive or X-linked modes of transmission.[4],[8]
Majourity of the patient shows a family history but there are patients for whom a family history cannot be identified.[8] AI affects both primary and permanent dentitions.
Clinically, AI appears as an alteration of enamel formation resulting in hypoplasia, hypocalcification, and hypomaturation. Enamel hypoplasia results in a decreased quantitative enamel formation. The enamel in hypocalcification appears normal but poorly mineralized while hypomaturation results in an abnormal mineralization in the final stages of tooth formation.[4],[8]
In the present case, composite veneering was the treatment of choice, as it was a minimally invasive treatment approach rather than full coverage restorations and also ceramic veneering was not the choice of treatment, as most of the teeth had very thin enamel or lack of enamel completely.
References:
1. Ozturk N, Sari Z, Ozturk B. An interdisciplinary approach for restoring function and esthetics in a patient with amelogenesis imperfecta and malocclusion: A clinical report. J Prosthet Dent 2004; 92:112-15.
2. Ravassipour DB, Powell CM, Phillips CL, Hart PS, Hart TC, Boyd C, Wright JT. Variation in dental and skeketal open bite malocclusion in humans with amelogenesis imperfecta. Archives of Oral Biology 2005; 50:611-23.
3. Witkop CJ Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J Oral Pathol 1988; 17:547-53.
4. Sengun A, Ozer F. Restoring function and aesthetics in a patient with amelogenesis imperfecta: A case report. Quintessence Int 2002; 33:199-204.
5. Robinson FG, Haubenreich JE. Oral rehabilitation of a young adult with hypoplastic amelogenesis imperfecta: A clinical report. J Prosthet Dent 2006; 95:10-13.
6. Alderd MJ, Savarirayan RC, Rawford PJ. Amelogenesis imperfect: a classification and catalogue for 21st century. Oral Disease 2003; 9:19-23.
7. Sari T, Usumez A. Restoring function and esthetics in a patient with amelogenesis imperfecta: A clinical report. J Prosthet Dent 2003; 90:522-25.
8. Weinmann JP, Svoboda, JF, Woods RW. Hereditary disturbances of enamel formation and calcification. J Am Dent Assoc 1945; 32:397-418.
|