Introduction
Cleft lip and palate is a congenital defect accompanied by varieties of dental and skeletal anomalies, including abnormalities in number, position, shape and occlusal development of teeth for e.g, supernumeraries, congenitally missing teeth, peg shaped teeth, natal teeth, enamel hypoplasia, germination, fusion, inverted teeth etc. An inverted tooth is a heterotopic tooth with roots towards the alveolar ridge[1]. Inverted tooth may also be associated with other conditions like odontogenic cysts, maxillary infections, trauma, lack of space and/or dense bone [2]. Inverted teeth most often develop due to disturbances causing an inverted location of the tooth bud [3].
Case
A 9-year old female patient named Lily Nayak reported to the Department of Pedodontics and Preventive Dentistry, S.C.B. Dental College, Cuttack with the chief complaint of pain in 85 for past 3 days. The patient was well developed with a history of hospitalizations for surgical repair of cleft lip and palate and presented with scars on the philtrum for the same.
Upon intraoral examination, there was a palatal scar, maxillary arch was narrow, left maxillary central incisor (21) was missing, right central incisor (11) was rotated and placed in the midline, oral hygiene was poor and there were multiple carious teeth. Examination by speech pathologist found language development to be normal with articulation marked by hyper nasality. On ENT examination, hearing was normal and a hard object was found in the right side nasal cavity.
Orthopantomograph (OPG) showed the left central incisor in the right side nasal cavity with the root developing towards the oral cavity. (Figure.1) The tooth was found to be inverted. The root was not completely formed. On further examination, the incisal edge of the same tooth was seen through the nasal mucosa (Figure.2). When palpated, the tooth was mobile and not firmly attached to the mucosa.
 | Figure-1 – Orthopantomograph
 |
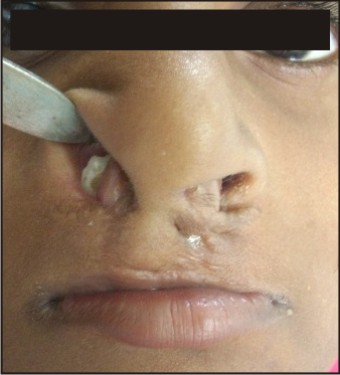 | Figure-2 - Intranasal Tooth
|
A proper treatment protocol was planned with pulpectomy in 85, extraction of nasally erupting 21under General anaesthesia through the nostril (Figure-3), extraction of 74, restoration of 75, orthodontic management of the malocclusion along with the required preventive schedule and prosthodontic rehabilitation thereafter. A plastic surgeon was consulted for repair of the oro-nasal communication at a later date as per the patient’s convenience.
 | Figure-3 - Extracted Tooth
|
Extraction of nasally erupting 21 and other procedures like pulpectomy and extraction were performed under General anaesthesia. Nasal pack was given. The patient was discharged after 3 days. Healing was uneventful and there was no post-operative complication.
Discussion
Cleft lip and palate is not uncommon, the prevalence being 1 in 800 live births[4]. Presence of intranasal teeth in these patients is 0.48% (0.24-0.85%)[5]. Intranasal teeth have also been reported very rarely in normal patients without clefts [6]. This can be a tooth of the normal series, either deciduous or permanent or a supernumerary tooth sometime[7]. Intranasal teeth cause symptoms like pain, discomfort, nasal discharge, posterior nasal dripping, headache, nasal obstruction, speech difficulties, sinusitis etc.[5],[8]. At times it can go unnoticed until a routine examination.
In almost all the cases reported, the treatment had been performed under general anesthesia, except for a case reported by Ozturk C. et al, who performed the extraction under Local Anesthesia [7]. In the present case, the root was more than half developed and tooth was not firmly attached to the nasal mucosa. So in this case also it was decided to remove the tooth under General anesthesia. There was no post-operative complication.
To conclude, Cleft lip and Palate patients present with many dental and skeletal anomalies, a rare one among which is intranasal teeth. The management is same in all cases i.e., extraction either under General or Local anesthesia and rehabilitation as needed.
References
1. Rãducanu AM, Cristea I, Feraru VI, Rãducanu MA. Dental Heterotopy- A clinical case report. OHDMBSC 2007;6(4):56-59.
2. Erkmen N, Olmez S, Onerci M, Supernumerary tooth in the maxillary sinus: case report. Ausralian Dental Journal 1996;43(6): 385-6.
3. Jacobs R, Willems G. Inverted eruption of a supplemental lower premolar: report of an unusual case. International Journal of Paediatric Dentistry 2003;13: 46–50.
4. Damle SG, Textbook of Pediatric Dentisrty. 3rd ed. New Delhi: Arya (medi); 2006.
5. Medeiros AS, Gomide MR, Costa B, Carrara CFC, Neves LTD. Prevalence of Intranasal Ectopic Teeth in Children with Complete Unilateral and Bilateral Cleft Lip and Palate. Cleft Palate–Craniofacial Journal May 2000;37(3):271-273.
6. Chen HC, Lee JC, Intranasal Tooth. J Med Sci 2005;25(5):255-258.
7. Ozturk C., Eryilmaz K.,Cakur B. Supernumerary tooth in the nose. Turk J Med Sci 2007;37(4):227-230.
8. Gupta YK, Shah N. Intranasal tooth as a complication of cleft lip and alveolus in a four year old child: case report and literature review. Int J Paediatr Dent. 2001 May;11(3):221-4
|