Introduction
Meyer-Rokitansky-Kuster-Hauser syndrome is characterized by congenital aplasia of the uterus and upper part (2/3rd ) of the vagina in women showing normal development of secondary sexual characteristics and a normal 46xx karyotype . It affects 1 out of 4500 women [1]. This syndrome is subdivided into two types .Type I(MRKH-isolated)or Rokitansky sequence and Type II(MURCS) mullerian duct aplasia Renal dysplasia and cervical somite anomalies. MRKH syndrome may also be associated with renal ,skeletal and more rarely cardiac and digital anomalies.The first clinical sign is primary amenorrhoea.[2] Treatment of this condition consists of creating a neovagina when the patient is ready to start sexual activity .It can be either surgical or non surgical depending on individual needs. Non surgical creation of neovagina includes application of dialator progressively increasing in length and diameter. Surgical treatment involves dissection of a space between the rectum and bladder and using a stent for vaginal dialation.
A Stent is an artificial mould inserted into a natural passage in the body to hold the cavity open .The name stent is originated from the name of Charles Stent an English dentist[3]. It is a device used in conjunction with a surgical procedure to keep a skin graft in place often modified with acrylic resin or dental modeling impression compound that was previously termed stent mass [4].
Case Report
A 19 year old girl reported to the Obstretics and Gynecology department in Pondicherry Institute of Medical Sciences,Pondicherry with primary amenorrhoea.She had normal height and weight and wa. All the vital signs were normal .The patient had rheumatic heart disease and Mitral regurgitation. On clinical examination the secondary sexual characteristics were well developed .Local examination revealed that the patient had thin labia majora and minora with sparse hair. Lower third of vagina was present and could be indented to 2 cm. The case was taken up for examination under anesthesia and diagnostic laparoscopy .
Laparoscopy showed normal ovaries with a luteal cyst in the right ovary. Both the fallopian tubes were present and met in the centre as a rudimentary uterus with no downward continuation. The patient was diagnosed with Meyer- Rokitansky -Kuster -Hauser syndrome .With the patient in lithotomy a space was created between the urethra anteriorly and rectum posteriorly . Haemostasis was assured and the patient had no post operative complaint. In order to prevent possible contracture of the reconstructed vagina a long term vaginal stent had to be placed to maintain width and depth and the case was referred to Dental department for a vaginal stent.
Clinical Procedure
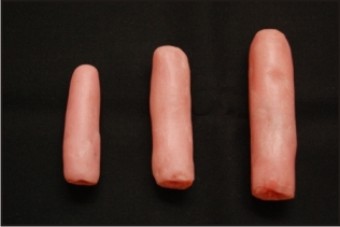
The approximate diameter of the neovagina was determined by digital palpation. A cylindrical acrylic mould was made with cold cure acrylic (DPI,RR,cold cure,Mumbai).The vaginal wall was lubricated with petrolatum and alginate impression material was applied on the acrylic model and was placed into the neovagina and held in position till the alginate was set..The cast was poured after boxing the impression with modeling wax. The tissue suface of the cast was lubricated and wax model was made with molten wax. The acrylic stent should be slightly larger than the diamension so that it can exert pressure laterally on the surrounding walls of the space to keep it patent. Cold cure acrylic is applied incrementally on the wax model and placed into the space and moulded.One end of the stent was rounded for easy penetration and not causing any damage to the surrounding mucosa.The other end was left open (Figure 1). The stent was polymerized by placing in warm water. Once the acrylic was polymerized and hardened it was placed in hot water and the wax inside was melted out. The open end of the stent was closed with an acrylic stop to prevent over insertion. The stent was trimmed and polished so that no rough surfaces was present as these could be the breeding ground for micro organisms.Proper placement of the stent was instructed to the patient with the use of a mirror. Initial diamension of the stent was 6cm lenth and 1.5cm diameter .The patient was recalled after 4 weeks for a stent of size 8cmx2cm.The size was gradually increased to a size of 10 cmx2.5 cm with 2 months intervals. (Figure 2). An attempt at sexual intercourse was suggested after the use of the last size stent for 2 months .Continued use was required if the intercourse was infrequent. The patient was also explained about surrogacy as an option after marriage. During the follow up period there was no hypertrophic scarring which may be seen at the apex of neovagina after Mc Indoe vaginoplasty . Adequate neovaginal depth was obtained with the stent.
 | Figure 1 :Hollow acrylic stent with one open end after removal of wax
 |
 | Figure 2: Hollow acrylic stent with a stop at one end
|
Care Of The Stent
The stent should be cleansed after use with antimicrobial agents like chlorhexidine and should be stored in antimicrobaial bath between uses. Hygiene is critical in the initial stages of healing.
Discussion
Uterus is normally formed from the mullerian duct in the 8 week old foetus .The two ducts meet at the centre caudally and the break down of the medial walls finally form the uterus and the upper 2/3rd vagina. The lower 1/3rd is f ormed from sinovaginal bulb [4].Diagnosis of MRKH syndrome is usually made at late adolescence as the patient presents with primary amenorrhoea [5]. M c Indoe vaginoplasty is one of the most preferred surgical intervention in mullerian agenisis[6]. A neovaginal cavity is created by dissecting between bladder and rectum . Inorder to prevent a possible contraction of the reconstructed vagina a long term vaginal stent use is required to maintain vaginal width and depth[7].
Several different materials have been used for vaginal stents.These include gauze,a glass dilator,candle wax,wood covered with condom,vulcanite and acrylic[8]. Customised acrylic strents help in preserving the depth of the cavity created. A hollow acrylic vaginal stent is of low weight and it remains stable and does not dislodge against gravity when in use.If the stent is of soft material the neovagina will be stretched less and it can result in a tapered neovagina. An acrylic stent provides the desired result.
Conclusion
A hollow acrylic vaginal stent can be used to maintain the patency of neovagina created in a case of Mayer- Rokitansky -Kuster -Hauser syndrome. Hollow acrylic stent which is of less weight is comfortable to use as well as can maintain the dialatation of the vagina. The smooth surface of the stent prevents microbial contamination on the appliance. It is an inexpensive to fabricate and easy to place stent which can be considered in a low resource set up. A vagina formed in this manner remains permanent in depth and caliber even if the patient neglects dilatation for more than a year.
References
1. Karina Mercel,Laura Camborieux,Daniel Guerici.Meyer Rokitansky Kuster Hauser syndrome.Orphanet Joyrnal ofRare Diseases,2007:2;13-15.
2. FolchM,PigemI,Konja JC.Mullerian agenesis etiology ,diagnosis and management .Obstrtret Gunecol Surv.2000,55;644-649.
3. Ring Melvin.How a dentist’s name became a synonym for a life saving disease .the story of Dr Charles Stent .Journal of history of Dentistry,2001:49(2);77-80.
4. The glossary of Prosthodontic terms.J Prosthet Dent<81:1;48-106.
5. John A Rock,Howard W Jones .Te Linde’s operative gynecology.9th ed,lippincott2003,710-716.
6. T G Blocker,SR Lewis ,C Snyder Plastic reconstruction of the artificial vagina .Journal of Plastic and Reconstruction Surgery.1953,11:3;177-182.
7. AyahanCoskun,Yusuf Kenen Coban,Mehmet Alivarda,,Ahmet Cemil Dalay.The use of silicone coated acrylic vaginal stent in Mc Indoe vaginoplasty and review of the literature concerning silicone based vaginal stent –A case report.BMC surgery.2007,7;13-17.
8. Mathew jain Connen ,H Croll,Charles .Plastic and reconstructive Surgery,91;2:367-368.
|