Introduction
Complete denture prosthesis being the fixed entity in dynamic oral environment does not remain closely adapted to underlying soft tissues owing toresidual ridge resorption and constantly occurring mucosal changes from muscle dynamics and tissue irritation[1]. An ideal denture base should be rigid enough to withstand the masticatory loads and flexible enough so that it continuously adapts to underlying soft tissues during function thus enhancing retention, better force distribution and patient comfort[2].
In 1961, Chase[3] reported application of elastic impression material on intaglio surface of denture to relieve abuse soft tissues.Since then,several materials including tissue conditioners and soft liners have been used on tissue surface of denture in cases with flabby ridges, atrophic residual alveolar ridges, denture sore mouth, xerostomics and diabetic patients. But these materials has proved to be a temporary alternative due to loss of by-products (plasticizers , alcohol) and encouragement of candidal growth over a period of time,thus requiring several relining visits and follow ups.
Treatment options for these patient’s include surgery, implant retained prosthesis or conventional prosthodontics without surgical intervention[4]. Treatment modality has to be chosen depending on patient’s state of health and need, extent of flabby tissue, financial capacity and skill of the dentist. In most situations, surgical intervention or use of implants is not possible and conservative management is the treatment of choice.Therefore, a more permanent solution for such cases can be liquid supported denture which has both plastic and elastic recovery.This case report describes technique of fabrication of liquid supported denture for flabby and atrophic maxillary edentulous residual alveolar ridge .
Case Report
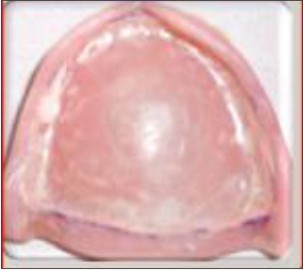
A 60 year old female patient was referred to Department of Prosthodontics, Sudha Rustagi College of Dental Sciences & Research, Faridabad, for prosthetic rehabilitation of completely edentulous maxillary and mandibular arches. Patient was known diabetic for the past 10 years and had been wearing dentures for the past 8 years.Patient complained of loosely fitting dentures especially during function and desired the replacement of the same.Intraoral examination revealed flabby atrophic anterior maxillary edentulous ridge (Image1). Orthopantographic examination revealed severe bone loss with respect to maxillary edentulous ridge (Image2). Hence, a liquid supported maxillary denture opposing conventional mandibular denture was planned for this particular patient.
 | Image 1: Intra Oral View of Flabby Atropic Maxillary Edentulous Ridge
 |
 | Image 2: OPG Showing Severly Resorbed Maxillary Ridge
|
Procedure
1) Primary impressions were made using Mc-Cords technique[5] by mixing 7 parts of green stick compound (DPI, Pinnacles) and 3 parts of impression compound (DPI).
2) Impressions were poured by dental plaster and diagnostic cast was obtained.Custom tray was fabricated and border moulding was performed using low fusing green stick compound. Final impression was made using light body polyvinylsiloxaneelastomeric impression material (Aquasil, Densply) and master cast obtained by pouring in dental stone.
3) Temporary denture base and occlusal rims were fabricated in usual manner and jaw relation was recorded.
4) Satisfactory trial was done and wax up of trial dentures was completed.
5) Mandibular denture was processed using heat cure acrylic resin (DPI Heat Cure) in conventional manner and finishing and polishing was done.
6) Following steps were followed for fabrication of liquid supported maxillary denture:
a. Soft and flexible vacuum heat pressed polyethylene sheet (Stavac, NY) of 1.5mm thickness was adapted on maxillary master cast 2mm short of sulcus using vacuum forming machine (Image3).
 | Image 3: 1.5 mm Thick, Polyethylene Sheet Vacuum Adapted Over The Master Cast & Incorporated During Packing Stage
|
b. Sheet was removed and trial denture was secured back on master cast and de-waxing was done in usual manner.
c. Adapted sheet was placed back on master cast and vaseline was applied on its surface for its easy retrieval and packing of denture mould was done using heat cure resin.
d. Denture with polyethylene sheet acting as a temporary spacer incorporated on tissue surface was processed using long curing cycle and finished and polished (Image4).
 | Image 4: 1.5 mm Thick Polyethylene Sheet Incorporated In The Final Denture
|
e. Denture insertion was done and checked for retention and stability and patient was asked to use the dentures till he got adapted to new dentures.
f. Maxillary complete denture was now ready to be converted into liquid supported denture:
Addition silicone putty impression (Aquasil, Densply)of the tissue surface of denture was made in an oversized stock tray and negative replica of tissue surface was obtained (Image5).
 | Image 5: Impression of Tissue Surface Made with Putty Impression Material & Positive Master Cast obtained
|
Junction of sheet and denture surface was marked on impression using marking pencil and dental stone was poured.Positive stone replica of tissue surface with marked junction was obtained (Image6).
 | Image 6: Positive stone replica of tissue surface with marked junction was obtained
|
Another soft and flexible permanentpolyethylene sheet of 0.5mm thickness was adapted on positive stone replica in same manner as explained for temporary polyethylene sheet.
Temporary polyethylene sheet(1.5mm) on denture surface is now removed carefully and replaced with thinner 0.5mm sheet for creating at least 1mm space for the liquid.
Junction of polyethylene sheet on tissue surface is carefully sealed using medical grade cynoacrylate to make it leak proof (Image7).
 | Image 7: 0.5 mm Polyethylene Sheet Adapted on the Intaglio Surface with the Junction Sealed using Medical Grade Cynoacrylate
|
Two holes of about 2mm diameter were made in disto-buccal region of denture and liquid glycerine was injected using needle and syringe through these inlets (Image8). After the space was filled completely, vertical dimension was checked and adjusted; junctions were again checked for leakage and holes were sealed off using cold cure resin.
Any sharp area was rounded off and dentures inserted (Image9,10). Post insertion instructions were given and denture hygiene instructions were reinforced.
 | Image 8: Glycerin is Injected Into the Tissue Surface
|
 | Image 9: Post operative Extraoral View
|
 | Image 10: Post Operative Frontal View
|
Follow up was carried out after 1 day, and then on weekly basis. Patient comfort was verified,and dentures were regularly checked for any glycerine leakage,retention and stability.
Discussion
In this patient, with atrophic maxillary edentulous ridge, liquid supported denture with its clear cut advantage of better retention, stability, support, and long term basal seat tissue preservation was planned. This unique design combines rigidity required on polished surface and flexibility required on tissue surface of denture continuously adapting to soft tissues during function and mastication. Liquid supported denture consists of pre-shaped flexible polyethylene sheet with glycerine acting as thin film of liquid in between denture base and foil. At rest, foil act as soft liner and during function vertical unidirectional forces gets evenly distributed over a larger surface area, resulting in optimal masticatory load distribution helping in long term basal seat tissues preservation. This modification in design clearly has advantages over conventional dentures which on the contrary have rigid polished as well as intaglio surface providing no adaptability with ever changing basal tissues whatsoever. Also has a role to play in distribution of stresses over wide area in patient having bruxism and enhanced masticatory dynamics, thus producing no sore spots enhancing patient comfort[6]. Liquid supported denture thus provides benefits of soft liners and tissue conditioners on long term basis.Polyethylene sheet was used in this particular case on tissue surface of denture due to its biocompatibility with oral tissue, flexibility, and favourable physical and mechanical properties.
Liquid medium used was nontoxic, clear, colourless,odourless glycerine which has proved to have good biocompatibility in vivo over the years.It also has good thermal stability, moisture repellency, low surface tension and vapour pressure and low cost.
Precaution
Denture base thickness should be at least 3 mm.
Junction of foil and denture surface should be hermetically sealed and regularly checked for leakage of liquid on follow up visits.
Post insertion instructions and denture hygiene instructions should be reinforced and followed strictly.
Patient should quickly make a dental visit to Prosthodontist for replacement of liquid in case of leakage.
Preserve the positive stone replica so that quickly sheet can be vacuum pressed on it in case of sheet damage or worn out.
Conclusion
Liquid supported denture with its combining rigidity and flexibility provides comfort, stability, retention and good adaptability of prosthesis in cases of bruxism, diabetes atrophic and flabby edentulous ridges, history of ridge soreness. De Vans dictum holds true in liquid supported denture cases as it provides long term preservation of hard and soft tissues .
References
1. D. A. Atwood. Post extraction changes in the adult mandible as illustrated by microradiographs of midsagittal sections and serialcephalometric roentgenograms.J Prosthet Dent, 1963;13(5):810-24.
2. D. Kakade, S. Athavale, S. Shingote, and B. Dammani. Liquid-supported denture: a gentle option. Journal of Indian Prosthodontist Society, 2007;7:35-9.
3. Chase WW. Tissue conditioning using dynamics adaptive stress. J Prosthet Dent 1961;11:804-15.
4. Crawford RW, Walmsley AD. A review of prosthodontic man- agement of fibrous ridges. Br Dent J 2005;199:715-9.
5. Mc Cord JF, Tyson KW. A conservative prosthodontics option for treatment of edentulous patients with atrophic(flat) mandibular ridges. Br Dent J 1997;182:469-72.
6. Boere G, Koomen HD, Davidson CL. Liquid supported dentures, Part II: Clinical study, a preliminary report. J Prosthet Dent 1989;62:434-6.
|