Introduction
The loss of a body part, especially one as visible as a finger or hand, can be emotionally upsetting. It may take time to adapt to changes in your appearance and ability to function. Talking about these feelings with your doctor or other patients who have had amputations often helps you come to terms with your amputation. You may ask your doctor to recommend a counsellor to assist with this process. It is important to remember that with time, you will adapt to your situation by finding new ways of doing your daily activities.
It is highly probable that a simple accident that will cause one to have a life-long lasting effect. an injury such as a loss of one finger is considered as a significant functional, life-long deficiency(michael& buckner 1994).
One way to restore the functionality of the lost digit is by replacing the
Amputation with prosthesis. According to michael & buckner (1994), prosthesis can restore a” near-normal function” of the original finger. Moreover, as long as 1cm of the mobile phalanxremains at the amputated region, the restoration of active grasp finger is feasible (ibid.).
The finger prosthesis are custom designed and hand made by a skilled artist using his own techniques in sculpting,and experience to imitate a living finger.to achieve this level of success,we need close contact with our patients.the first visit will last approximately 3 hours as impressions, photos and measurements will be taken in order to match the skin tone and nail shape.the prosthesis will have a matching finger print, veins and freckles.
Case Report:
A 24 year old patient reported to the department of prosthodontics, navodaya dental college, raichur for the replacement of his missing finger.
On examination it was noticed that patient had lost part of his index finger due to trauma caused while he was working on a spinning machine.the amputated finger showed thickened ends,surrounding area appeared to be normal with no signs of any pathology in relation to other digits.
On complete examination of the amputated finger it was seen that a residual stump,dark brown in colour on the index finger of the right hand measuring 3.5cm in height.
The case was discussed and methods to replace the finger was formulated .two different treatment plans was discussed with the patient.
One of the treatment plan was fabrication of finger prosthesis with industrial silicone the other treatment plan was implant retained finger prosthesis.
Implant retained finger was not considered due to financial constraints so it was decided to fabricate a finger prosthesis with industrial silicone.
As a part of routine treatment planning and to ensure the patients willingness and co operation and informed consent was signed before beginning the treatment .
Prosthetic Solution
The fabrication of the prosthesis included designing of the sleeve was pattern followed by lab procedures to fabricate it into a silicone prosthesis.
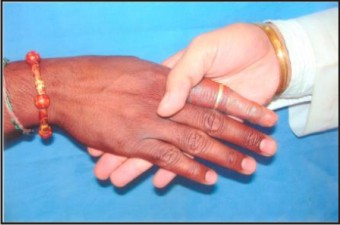
(A) The right hand was lubricated with a superficial layer of petroleum jelly to prevent adherence of impression material to the skin and hair. (Fig 1 & 2).
 | Fig 1:Preoperative View
 |
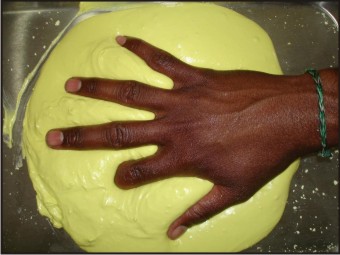 | Fig 2:Impression Making
|
(B) The right hand and the left index finger was duplicated in a hydrocolloid impression material and the impression was replicated with dental stone. (Fig 3).
 | Fig 3:Retentive Clips On Impression
|
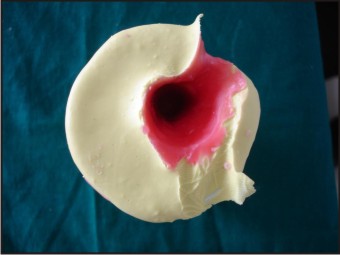
(C) A separate impression of the amputated finger was made and a corresponding stump of the same was made with dental stone. (Fig 4).
 | Fig 4:Pouring Of Model
|
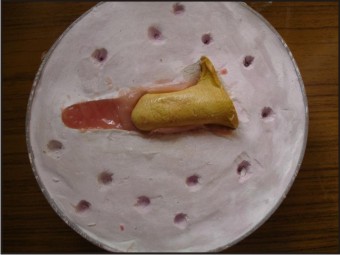
(D) Wax pattern of the left index finger was made to simulate the amputated right index finger. (Fig 5).
 | Fig 5:Wax Pattern
|
(E) Investmenttechnique: the wax pattern of the left index finger was invested .then dewaxing of the same was done.
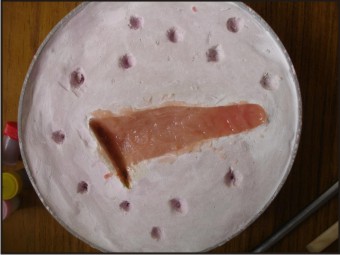
(F) The stump of the right amputated finger was placed in the mould. (Fig 6).
 | Fig 6:Stump Model
|
(G) Different intrinsic stains was placed over a porcelain tile ,incrementally stains were incorporated into the silicone material and mixed shade matching was done by placing the increments of silicone material in a cellophane sheet and matched with dorsal surface as well as the ventral surface of the left index finger. (Fig 7 & 8).
 | Fig 7:Shade Selection
|
 | Fig 8:Shade Matching
|
(H) After shade matching the silicone material was packed for the dorsal surface first then the stump was incorporated into the mould .later in the ventral surface was proceed with silicone material. (Fig 9, 10, 11, 12).
 | Fig 9:Packing Of Indusrtrial Silicone Dorsal Surface
|
 | Fig 10:Packing Of Indusrtrial Silicone Dorsal Surface
|
 | Fig 11:Packing Of Indusrtrial Silicone Ventral Surface
|
 | Fig 12:Packing Of Indusrtrial Silicone Ventral Surface
|
(I) The material used in the prosthesis was industrial silicone .the material was left for 24 hours as per the manufacturer instructions to complete the curing cycle of the material.
(J) The finishing of the prosthesis was done after 24 hours with tungsten carbide burs. (Fig 13).
 | Fig 13:Cured Prosthesis
|
(K) The final prosthesis was delivered and the fit and colour of the final prosthesis was evaluated and was found to be satisfactory. (Fig 14).
 | Fig 14:Postoperative
|
Discussion:
The amputation of one or more fingers of the hand ,as the consequence of trauma or congenital absence of one or more phalanges ,carries a serious reduction of hand function and social dysfunction for the patient.Many injuries and traumatic amputations of fingers can be rescued by microsurgery through re-implantation. however it may not be advisable or possible in some cases such as the patient’s unwillingness or factors such as cost.[1]
Prostheses for the upper limb have been broadly classified as functional and aesthetic .the patient may be treated with the surgical or non surgical approach .as the patient was not willing to bear any expenses ,a non surgical method of rehabilitation was carried out. aesthetic prosthesis has been defined as passive devices aimed at restoring normal appearance of the hand, but silicone rubber has proved to be the most promising in achieving the desired life like effects .the acceptance of prosthesis has been much higher with the use of custom restoration using silicone elastomer.[1]
Almost all stains,including ballpoint ink,newsprint,clothing dyes,and food colourings can be removed easily with water and soap.
The gentle ,constant pressure of elastomer prosthesis can help densensitize and protect the injured tip.[1]
The fit of the finger prosthesis is another important concern of the patients – a tight fit causes discomfort while a loose fit can cause embarrassment if the prosthesis fall off in public.[3]
The skin of the hand also changes color therapy and application and meticulous attention to detail.[3]
With the use of modern materials, improved methods of fabrication and attention to detail ,a high quality cosmetic result can be achieved .all patients were concerned primarily with the cosmetic appearance of the hand and function was a secondary consideration.[2]
Recent literature speculates that silicone gel improves the hydration of the stratum corneum of immature hypertrophic scars.[1], [2], [3], [4]
Post Rehabilitation To The Patient:
1. Before Placing The Prosthesis Apply A Thin Layer Of Water Base Lubricant To The Underlying Skin And Gently Place The Prosthesis.
2. Do Not Wear The Prosthesis Overnight As It May Cause Irritation To The Skin.
3. Wash Prosthesis Everyday With A Mild Soap.Avoid Exposure Of Prosthesis To High Temparture
References:
1. Ashwini Y Kini,Preeti P Byakod,Gangadhar S Angadi,Umesh Pai.Comprehensive Prosthetic Rehabilitation Of A Patient With Partial Finger Amputations Using Silicone Biomaterial:A Technical Note.Prosthetics And Orthotics International Dec 2010;34(4):488-494.
2. M.J Pilley ,D.N Quinton.Digital Prosthesis For Single Finger Amputations.Journal Of Hand Surgery (British And European Volume,1999)24b:5:539-541
3. Shivani Kohli,Shekhar Bhatia,Nishita Garg,Abhay Kumar Jain,Akram Ansari,Jaspal Singh.Case Report –Patient Specific Prosthetic Rehabilitation Of Finger And Eye.Indian Journal Of Dentistry 2011;2;3.
4. Nshanmuganathan, M. UmaMaheswari, V.Anandkumar, T.V. Padmanabhan. J Indian Prosthodont Soc(Oct-Dec 2011)11(4);232-237.
|