Introduction
Dentigerous or follicular cysts are the second most common type of odontogenic cysts, and the most common developmental cysts of the jaws.[1] The dentigerous cyst is defined as a cyst that originates by the separation of the follicle from around the crown of an unerupted tooth.[2] Dental follicle associated with unerupted or impacted teeth shows fibrous connective tissue with remnants of reduced enamel epithelium. Dentigerous cysts are caused by expansion of dental follicles resulting from accumulation of fluid between tooth crowns and epithelial components.[3] It occurs most commonly in the second and third decade of life and typically involves the mandibular third molar, the maxillary canines and the mandibular premolars followed by supernumerary teeth and the central incisor in the decreasing order of the frequency of involvement.[4] Only5% of dentigerous cysts are associated with supernumerary teeth. The usual age of clinical presentation of dentigerous cyst due to supernumerary tooth is in the first four decades of life.[5] We report a case of dentigerous cyst associated with impacted mesiodens in a 19 year old male patient.
Case Report
A 19 year old male patient reported to the department with chief complaint of swelling since 1 month and pain since 5 days in the right maxillary anterior region. The swelling had gradually increased to present size which was associated with pain which was dull, intermittent, nonradiating in nature, does not aggravate on taking food and gave no history of taking medication. He did not give history of any trauma. On general examination, the patient was apparently healthy and there was no history of systemic diseases. Thevital signs were within normal limits.
On extra oral examination a solitary diffuse swelling present irt right middle third of face measuring of about 2cm X 1.5cm in size extendingmediolaterally from philtrum of lip to the corner of mouth with obliteration of right nasolabial fold and superoinferiorly extending from 2 cm inferior to the right inner canthus of the eye to the inferior border of the upper lip (Fig 1 & 2). The skin over the swelling appears to be normal. On palpation, there was no local rise in temperature. The swelling was soft to firm in consistency, tender on palpation, non fluctuant and not fixed to surrounding structures.On intra oral examination irt labial aspect, a solitary diffuse intraoral swelling measuring about 1.2cm X 1.5cm, roughly oval in shape was seen in the maxillary anterior labial vestibule extending from the right central incisor up to the right first premolar (Fig 3). The mucosa over the swelling appears to be normal. On palatal aspect, a solitary diffuse swelling measuring about 2cm X 2.5cm was seen irt right anterior region of hard palate extending mediolaterally from midpalatine raphe to 1cm away from palatal gingiva and anteroposteriorly extending from right central incisor up to the right first premolarand mucosa over the swelling appears to be normal (Fig 4). On palpation, the swelling was soft to firm in consistency, tender on palpation and obliteration of labial vestibule and expansion of cortical plate was present. Vitality test was done for all the right maxillary anterior teeth which elicits delayed response irt the right central incisor. Based on the history and clinical examination a provisional diagnosis of the infected radicular cyst irt right maxillary central incisor for which differential diagnosis dentigerous cyst, adenomatoid odontogenic tumor, calcifying cystic odontogenic tumor irt maxillary anterior region was given.
On radiographic examination, intraoral periapical radiograph irt right maxillary canine and anterior maxillary occlusal radiograph reveals a well defined radiolucent lesion in the right anterior maxillary region measuring about 1.5cm X 2 cm with sclerotic borders and lesion was extending in between the roots of right central incisor and lateral incisor causing displacement of roots with conical shape tooth present horizontally in the radiolucent lesion. There is widening of periodontal ligament space and loss of lamina dura irt 11 to 13 regions (Fig 5, Fig 6).
The digital panoramic radiograph showed a well-circumscribed radiolucent lesion in the right maxillary anterior region with conical shape tooth present horizontally in the radiolucent lesion (Fig 7). The aspiration yields straw colored fluid (Fig 8). The smear shows desquamated epithelial cells, mixed inflammatory cells like neutrophils, macrophages, lymphocytes and plasma cells in an eosinophilic background suggestive of inflammatory cystic lesion. The root canal treatment was done irt right maxillary central incisor, lateral incisor and canine. The lesion was surgically enucleated under local anesthesia along with the removal of the supernumerary tooth (Fig 9). The specimen was sent for histopathological examination. The haematoxylin & eosin stained section shows cystic epithelium overlying a connective tissue capsule. The epithelium is nonkeratinized with 2- 3 cell layer thickness. The cells are flat with hyper chromatic nucleus. The connective tissue is highly collagenized, with plenty of mixed inflammatory cells, dilated blood vessels and extravasated red blood cells with features suggestive of inflamed dentigerous cyst (Fig 10). The final histopathology report confirmed the diagnosis of inflamed dentigerous cyst.
 | Fig 1 : Mediolateral Extension Of Swelling
 |
 | Fig 2 : Superoinferior Extension Of Swelling
|
 | Fig 3 : A Diffuse Swelling In The Labial Vestibule
|
 | Fig 4 : A Diffuse Swelling Over The Right Anterior Region Of Hard Palate.
|
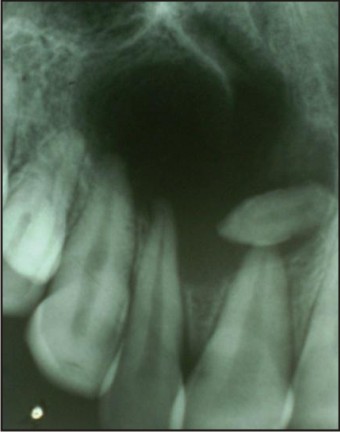 | Fig 5 : Iopa Radiograph
|
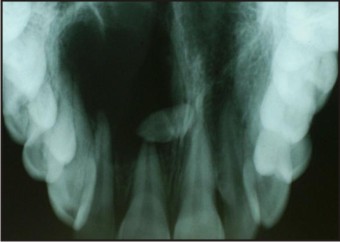 | Fig 6 : Anterior Maxillary Occlusal Radiograph
|
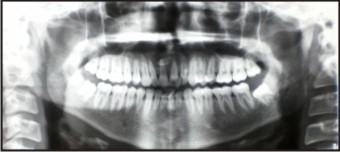 | Fig 7 : Digital Panoramic Radiograph
|
 | Fig 8 : Straw Colored Fluid
|
 | Fig 9 : Surgically Excised Tissue Along With Supernumerary Tooth.
|
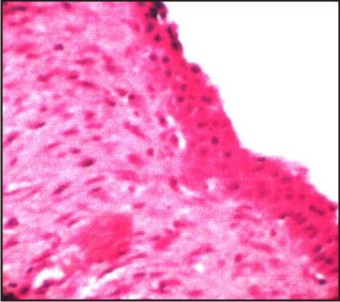 | Fig 10 : The Haematoxylin & Eosin Stained Section Shows Cystic Epithelium Overlying A Connective Tissue Capsule
|
Discussion
The word dentigerous means “tooth bearing” which describes the cyst appropriately. There are three primary variants of dentigerous cyst based on the location of cyst with respect to the erupting tooth: a) the eruption cyst; b) circumferential dentigerous cyst; c) lateral dentigerous cyst.[1], [6] According to pathogenesis dentigerous cyst are of two types: the first is developmental in origin and occurs in mature teeth usually as a result of impaction. The second type is inflammatory in origin and occurs in immature teeth as a result of inflammation from nonvital deciduous tooth follicle.[7]
Dentigerous cysts are often asymptomatic and are usually diagnosed during routine radiographic examination. The diagnosis relies on the radiographic and surgical observation of the attachment of the cyst to the cementoenamel junction.[8] They can enlarge causing bone expansion, erosion, pathological fractures or may become secondarily infected. The expansion of dentigerous cyst is related to a secondary increase in the cyst fluid osmolality as a result of the passage of the inflammatory cells and desquamated epithelial cells into cyst lumen. Swelling, tooth displacement, tooth mobility and sensitivity may be present if cyst reaches a size larger than 2cm in diameter.[9]
A cystic swelling of the hard palate may be the result of different kinds of cysts: odontogenic, non odontogenic or bone cysts. The studies have shown that the incidence rate of dentigerous cyst involving maxillary central incisor is 1.5% as compared to 45.7% involving the mandibular third molar.[7] In our patient dentigerous cyst caused by mesiodens may be the cause of swelling in labial and hard palate region. Hence it should be carefully differentiated from other mid palatal swellings. The etiology of supernumerary teeth is unknown. Supernumerary teeth are most common in the maxilla with a strong predilection for the anterior region; in which case the supernumerary tooth is termed a mesiodens.[3] A mesiodens has an overall prevalence of 0.15-1.9%. A mesiodens can occur individually or in multiplesand often does not erupt.[5] The presence of mesiodens causes complications such as delayed eruption of permanent teeth, rotations, retention, root resorption, pulp necrosis and diastema as well as formation of dentigerous and primordial cysts. Dentigerous cyst formation is another problem that may be associated with supernumerary teeth. Primosch reported an enlarged follicular sac in 30% of cases, but histological evidence of cyst formation was found in only 4 to 9% of cases.Resorption of roots adjacent to a supernumerary may occur but it is extremely rare as in our patient resorption of root was not observed.[10]
Radio graphically, the dentigerous cyst typically appears as a well-circumscribed, unilocular, usually symmetric radiolucency around the crown of an impacted tooth. The internal aspect of the cyst iscompletely radiolucent except for the crown of the involved tooth. One of the most difficult conditions to distinguish in the differential diagnosis is hyperplastic follicle. Other conditions that must be excluded in the diagnosis are odontogenic keratocyst, ameloblastic fibroma, and cystic ameloblastoma.[11],[12],[7]
Scolozzi et alreported an unusual case of a large dentigerous cyst associated with an impacted mesiodens, resulting in a slow-growing swelling in the upper lip. Khan et alalso described an upper lip swelling caused by a large dentigerous cyst associated with mesiodens. Dinkar et aldescribed an unusually early presentation of multiple mesiodens with associated dentigerous cyst. Large dentigerous cysts arising from unerupted mesiodens should be kept in mind in the differential diagnosis of upper lip swellings, particularly if associated with dental anomalies of the maxillary incisors such as malposition and diastema.[3] Asaumi et al reported a prevalence of 11% and suggested that mesiodens impacted for prolonged periods of time possess a higher risk of forming dentigerous cysts.[13]
Treatment of choice for dentigerous cysts is surgical removal. The standard treatment for a dentigerous cyst is enucleation and extraction of the cyst associated impacted or unerupted tooth. However, large lesions can be marsupialised. Because of the potential for occurrence of an odontogenic keratocyst or the development of an ameloblastoma or mucoepidermoid carcinoma all such lesions when removed, should be submitted for histopathological evaluation.
Conclusion
Even though a dentigerous cyst associated with impacted permanent teeth is not uncommon, such development as a result of an impacted supernumerary tooth might be rare. Therefore, supernumerary teeth should be examined carefully to prevent harmful effects on the adjacent regular teeth and possible cystic development.
References
1. Langlais RP, Langland OE and Nortje CJ. Diagnostic imaging of the jaws. USA: Waverly Company;1995:286-291.
2. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 3rd ed. St. Louis: Saunders; 2008:679-81.
3. Sepideh Vosough Hosseini, Monir Moradzadeh, Mehrdad Lotfi, Amir Ala Aghbali, Shirin Fattahi. Dentigerous Cyst Associated with a Mesiodens: A Case Report Journal of Dental Research, Dental Clinics, Dental Prospects 2011;5:76-78.
4. John T, Guna Shekhar M,et al. Dentigerous Cyst Associated With Supernumerary Teeth.Report of Three Cases Journal of Clinical and Diagnostic Research. 2010;4:2601-2606.
5. Grover SB, Singh P, Venkatachalam VP, Hekha N. Mesiodens presenting as a dentigerous cyst: case report. Indian J Radiol Imaging 2005;15:69-72.
6. Worth H.M. Principles and practice of oral radiographic interpretation. Chicago: Year Book Medical Publishers; 1975:466-472.
7. Shear M. Dentigerous (follicular) cyst. In cysts of the oral region, 2nded. Bristol: Weight PSG;1983:56-75
8. Dinkar AD, Dawasaz AA, Shenoy S. Dentigerous cyst associated with multiple mesiodens: a case report. J Indian Soc Pedod Prev Dent 2007;25:56-9.
9. Baranwal HC, Pushpendra Kumar Verma, Dwivedi CD, Srivastva Ruchi. Dentigerous cyst associated with animpacted maxillary mesiodens. European Journal of General Dentistry 2012;1:50-53.
10. Garvey MT, Barry HJ, Blake M. Supernumerary Teeth -An Overview of Classification, Diagnosis and ManagementJ Can Dent Assoc 1999;65:612-6.
11. Von Arx T. Anterior maxillary supernumerary teeth: a clinical and radiographic study. Aust Dent J 1992;37:189-95.
12. Daley TD, Wysocki GP. The small dentigerous cyst. A diagnostic dilemma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:77-81.
13. Asaumi JI, Shibata Y, Yanagi Y, et al. Radiographic examination of mesiodens and their associated complications.Dentomaxillofac Radiol 2004;33:125-27.
|