Introduction
Class III malocclusions are considered to be among the most challenging malocclusions to treat because of the unpredictable and potentially unfavorable nature of growth in patients with this skeletal pattern. Skeletal class III malocclusion is characterised by maxillary undergrowth, mandibular overgrowth or the combination of both conditions. Studies have shown that greater prevalence of skeletal class III malocclusion in subjects of Asian ancestry[1],[2] (4-19%) in comparison to European and north American ancestry [3],[4] (0.02- 12%).
The influence of the soft tissues on craniofacial growth has been discussed in the orthodontic literature for many years. Because of the close relationship between the pharynx and the dentofacial structures, a mutual interaction is expected to occur between the pharyngeal structures and the dentofacial pattern, and therefore justifies orthodontic interest. It has been demonstrated that there are significant relationships between the pharyngeal structures and both dentofacial and craniofacial structures at varying degrees.[5] It has been also suggested that skeletal class III with maxillary hypoplasia is a cause of upper pharynx constriction.[6]
Maxillary advancement by reverse headgear has been considered a major treatment option in young growing patients.[7],[8] Many studies demonstrated that maxillary advancement by reverse headgear stimulates the forward displacement of maxilla; reduce forward displacement of mandible, clockwise rotation of the mandible, retroclination of mandibular incisors and proclination of maxillary incisors.[8],[9],[10],[11] Although many studies have reported the skeletal and dental changes associated with treatment using reverse headgear, but only a limited number of studies have been reported on the relationship between maxillary protraction and pharyngeal size.[12],[13] It has been reported that saggital airway dimensions could be increased by the stimulation of forward maxillary growth, but only short term treatment results have been reported on relationship between maxillary protraction and airway size. Thus the purpose of this study was to investigate the long term effects of treatment with reverse headgear in patients with anterior cross bite and skeletal class III malocclusion due to maxillary deficiency on sagittal pharyngeal dimensions.
Materials And Methods
The sample consisted of 21 patients (8 boys and 13 girls) who were treated with a reverse headgear appliance. The patients were selected in the study based on the following inclusion criteria:-
1. Skeletal class III malocclusion with maxillary skeltal retrusion.
2. Comprehensive medical and dental history ruling out any systemic illness.
3. Patient with no history of previous orthodontic treatment.
4. An anterior crossbite with a Class III molar relationship.
5. No mandibular displacement.
In order to obtain a forward movement of the maxilla and maxillary dentition during the treatment period, elastic forces were applied between the face mask and the hook which were given in the acrylic splint between the maxillary canine and lateral incisors .The splint was cemented to maxillary arch with a minimum thickness sufficient to open the bite to an edge to edge incisal position.
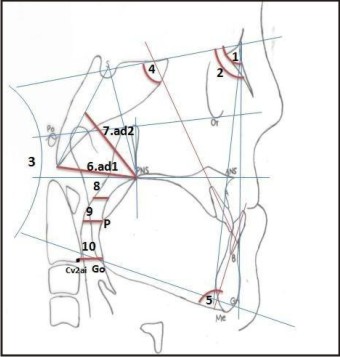
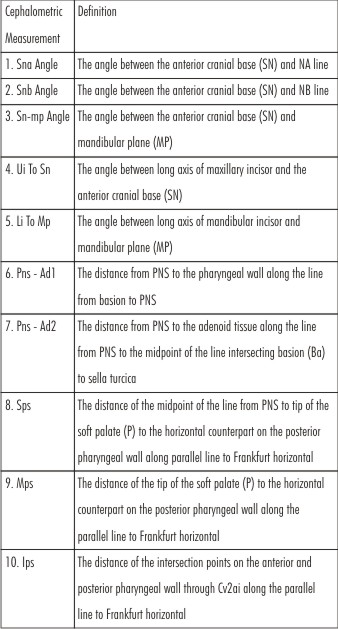
The magnitude of protraction force was approximately 400 gram per side and its direction was 30 degrees downwards from occlusal plane. The patients were instructed to wear the appliance 16 hrs per day. All the patients were treated until a normal overjet , class I molar and canine relationship was obtained. The patients were then placed on Frankel appliance for 6 to 9 months. The mean age of the subjects at T1 was 8.4years ± 1.1 years, and 10.6 years±1.6 years at T2.Treatment changes were evaluated on lateral cephalograms at T1 (pre treatment) and T2 (post treatment after Frankel appliance wear for 6 to 9 months). While recording the lateral cephalograms, patients were placed in standing position with the FH plane parallel to the floor and the teeth in centric occlusion. All of the cephalograms were recorded in the same machine with the same exposure parameters .Values at T1 and T2 and the difference between the two values were evaluated for each variable .Reference point and cephalometric variables used in study for linear and angular measurements are shown in Fig. 1 and Table 1.
 |
 |
 |
|
Results
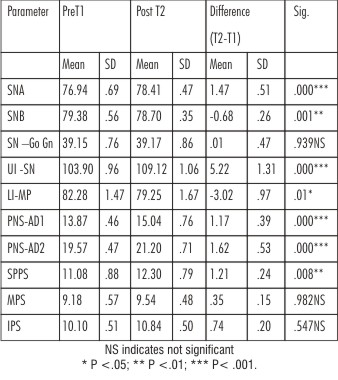
The mean and stsnderd deviation of each cephalometric variable at T1 and T2 and of difference between (T2-T1) were statisticaly analysed using paired t-test and results are presented in Table 2.
 |
|
The mean value of SNA significantly increased from 76.94±.69 to 78.41±.47 degrees and SNB significantly decreased from 79.38±.56 to 78.70±.35degrees.
The mean value of SN-MP (Go-Gn) increased from 39.15 ± .76 to 39.17 ± .86 degrees from T1 to T2 . The mean value of UI to SN increased from 103.90±.96 to 109.12 ± 1.06 degrees which was statisticaly significant and indicated proclination of of maxillary incisors, whereas mean value of LI to MP significantly decresed from 82.28 ± 1.47 to 79.25± 1.67degrees indicating lingual tipping of lower incisors. As for airway space measurement PNS- ad1 increased by13.87 ± .46 to 15.04 ± .76 mmand PNS ad-2 incresed by19.57± .47 to 21.20 ±.71mm which were statistically significant. SPS increased from 11.08 ±.88to 12.30± .79 mm.
Discussion
This study evaluated the effects of face mask followed by frankel appliance on the skeletal morphology and upper airway dimensions in subjects with skeletal class III malocclusion. Early treatment with maxillary protraction appliance can produce good results in patients having skeletal class III malocclusion with maxillary deficiancy. Treatment with face mask results in forward displacement of maxilla and maxillary teeth and reduces the forward displacement of mandible.[8],[9],[10],[14]
The duration of daily face mask wear in the literature varied from 8-16 hours with a force between 400-1200 grams for 4-16 months.[8],[9],[10],[11],[14]. In the present study the patients were requested to wear their appliances for 16 hours a day, and forces of 400 grams were applied on each side .The Face mask thepay was discontinued after the positive overjet and class I molar relationship is achieved and the patient were placed on Frankel appliance FR III for six to nine months.
The treatment changes were determined using lateral cephalometric radigraphs. Many limitations of the lateral cephalograms have been discussed[15] particularly inadequate description of airway in a two-dimensional radiograph. Measurements in airway space, tongue and hyoid bone using lateral cephalometric radiographs were known to have a correlation with those using CT [16]. The use of lateral cephalograms for the airway analysis is an established tool.[17] Reproducibility of airway dimensions on lateral cephalograms was found to be highly accurate.[18] Although three-dimensional imaging would be the appropriate method for the evaluation of pharyngeal airway dimension, the technique is not available in all centres and results in a relatively high radiation dose.[19] Therefore; the conventional lateral cephalogram remains a valuable and reliable diagnostic tool in numerous airway studies.
The face mask affected both the maxilla and mandible .Significant increases were measured in SNA (p<.001), indicating saggital movement of upper jaw ,whereas significant decrease was observed in SNB angle (p<.001). These results are compatible with the results regarding maxillary protraction in the literature. [8],[9],[10],[11],[14]
In addition to the skeletal changes concomitant effects of face mask on the dentition can not be avoided because the teeth provide the support for appliance. In the present study maxillary incisors were tipped labially by 5.22±1.31 which is simmilar to reported by Hiyama et al [20] (6.2±6.6) but more than reported by Kim et al[21] (mean 2.8). Mandibular rotational changes as demonstrated with change in SN – MP angle were not significant statistically. This was in contrast to the findings of Oktay and Ulukaya[12] and Hiyama et al[20] who reported a significant clockwise rotation of mandible after maxillary protraction.
In the present study measurement of nasophharyngeal space showed an increase after the treatment with face mask, where PNS -ad1 and PNS- ad 2 were increased by 1.17±.39 and 1.62±.53 respectively. These results were in consistent with the results of Sayinsu et al,[22] Kaysinigz et al[23] and Lee et al[24] which showed an increse in nasopharyngeal space. Lee et al[24] reported a positive corelation change in PNS ad1 (r=.529)and PNS ad 2 (r=.483) with changes in maxillary unit length, indicating that maxillary growth with maxillary protraction appliance caused increased nasopharyngeal space. Mucedero et al[25] in a study evaluating effects of maxillary protraction with or without expansion on the sagittal pharyngeal dimensions in class III subjects did not find any significant changes in oropharyngeal and nasopharyngeal airway dimensions. These findings were against the findings in our study and may be due to the fact that Hawleys retainer was used in the maxilla after active therapy whereas we used Frankel appliance for 6-9 months after active therapy.
In the present study there was a signicant increse in the superior oropharyngeal space (SPS) simmilar to reported by Kaygisiz et al[23]. Ceylan and Oktay[5] reported that oropharyngeal space decreased with the increase in ANB angle. Akcam et al[26] reported that airway space decreased in patients with clockwise rotation of mandible. In this study small clockwise rotation of mandible did not cause the reduction of oropharyngeal space. Changes in middle and inferior pharyngeal (MPS and IPS) spaces were not significant statistically, which is in accordance with the studies of Hiyama et al[20] and Kaygisiz et al.[23]
In the present study maxillary protraction applinance produced significant increase in in the upper airway space ,especially at the nasophyranx. Based on these findings maxillary protraction treatment could contribute to an increase in upper airway dimension and improve the respiratory function in patients with maxillary hypoplasia.
Conclusion
Treatment in class III patients with face mask in growing patients results in improved nasopharyngeal and oropharyngeal airway dimensions apart from forward movement of the maxilla.
References
1. Tang E. Prevalence of malocclusion amongst Hong Kong male dental students. Br J Orthod 1994; 21:57-63.
2. Baik H, Han H, Kim D, Proffit W. Cephalometric characteristics of Korean Class III surgical patients and their relationship to plans for surgical treatment. Int J Adult Orthod Orthognath Surg 2000; 15:119-28.
3. Kelly JE, Harvey C. An assessment of the teeth of youths 12-17 years. DHEW Publication No (HRA) 77-1644. Washington, DC: National Center for Healt Statistics; 1977.
4. Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the N-HANES III survey. Int J Adult Orthod Orthognath Surg 1998; 13:97-106.
5. Ceylan I, Oktay H. A study of the pharyngeal size in different skeletal patterns. Am J Orthod Dentofacial Orthop. 1995; 108:69–75.
6. Mermigos J, Full CA, Andreasen G. Protraction of the maxillofacial complex. Am J Orthod Dentofacial Orthop. 1990; 98:47–55.
7. Kapust AJ, Sinclair PM, Turley PK. Cephalometric effects of face mask/expansion therapy in Class III children: a comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998; 113:204–212.
8. Bacetti T, McGill JS, Franchi L, McNamara Jr JA, Tollaro I. Skeletal effects of early treatment of Class III malocclusion with maxillary expansion and face-mask therapy. Am J Orthod Dentofacial Orthop. 1998; 113:333–343.
9. Gallagher RW, Miranda F, Buschang PH. Maxillary protraction: treatment and posttreatment effects. Am J Orthod Dentofacial Orthop. 1998; 113:612–619.
10. Yu¨ksel S, Uc¸em TT, Keykubat A. Early and late face mask therapy. Eur J Orthod. 2001;23:559–568.
11. Sung SJ, Baik HS. Assessment of skeletal and dental changes by maxillary protraction. Am J Orthod Dentofacial Orthop. 1998; 114:492–502.
12. Oktay H, Ulukaya E. Maxillary protraction appliance effect on the size of the upper airway passage. Angle Orthod. 2008; 78:209–214.
13. Kılınc AS, Arslan SG, Kama JD, Ozer T, Darı O. Effects on the sagittal pharyngeal dimensions of protraction and rapid palatal expansion in Class III malocclusion subjects. Eur J Orthod. 2008; 30:61–66.
14. Ngan P, Hagg U, Yiu C, Merwin D, Wei SH. Treatment response to maxillary expansion and protraction. Eur J Orthod.1996; 18:151–168.
15. Finkelstein Y, Wexler D, Horowitz E, et al. Frontal and lateral cephalometry in patients with sleep-disordered breathing. Laryngoscope. 2001; 111:634–641.
16. Lowe AA, Fleetham JA, Adachi S, Ryan CF. Cephalometric and computed tomographic predictors of obstructive sleep apnea severity. Am J Orthod Dentofacial Orthop. 1995; 107:589–595.
17. Battagel JM, Johal A, Kotecha B. A cephalometric comparison of subjects with snoring and obstructive sleep apnea. Eur J Orthod. 2000; 22:353–365.
18. Malkoc S, Usumez S, Nur M, Donaghy CE. Reproducibility of airway dimensions and tongue and hyoid positions on lateral cephalograms. Am J Orthod Dentofacial Orthop. 2005; 128:513–516.
19. Jena AK, Singh SP, Utreja AK. Effectiveness of twin-block and Mandibular Protraction Appliance-IV in the improvement of pharyngeal airway passage dimensions in Class II malocclusion subjects with a retrognathic mandible.Angle Orthod.2013; 83:728-34.
20. Hiyama S, Suda N, Ishii-Suzuki M, Tsuiki S, Ogawa M, Suzuki S, Kuroda T. Effects of maxillary protraction on craniofacial structures and upper-airway dimension. Angle Orthod. 2002; 72:43–47.
21. Kim JH, Viana MAG, Graber TM, Omerza FF, BeGole EA. The effectiveness of protraction face mask therapy: A meta-analysis. Am J Orthod Dentofacial Orthop. 1999; 115:675–685.
22. Sayinsu K, Isik F, Arun T. Sagittal airway dimension following maxillary protraction: a pilot study. Eur J Orthod 2006; 28:184-9.
23. Kaygisiz E, Tuncer BB, Yu¨ ksel S, Tuncer C, Yildiz C. Effects of maxillary protraction and fixed appliance therapy on the pharyngeal airway. Angle Orthod. 2009; 79:660–667.
24. Lee JW, Park KH, Kim SH, Park YG, Kim SJ. Correlation between skeletal changes bymaxillary protractionand upper airway dimensions. Angle Orthod;2011; 81:426- 32.
25. Mucedero M, Baccetti T, Franchi L, Cozza P. Effects of maxillary protraction with or without expansion on the sagittal pharyngeal dimensions in Class III subjects. Am J Orthod Dentofacial Orthop. 2009; 135:777–781.
26. Akcam MO, Toygar U, Wada T. Longitudinal investigation of soft palate and nasopharyngeal airway relations in different rotation types. Angle Orthod. 2002;72:521–526.
|