|
|
|
| A New Dynamic Jaw Exerciser |
Bhawana Tiwari 1 , Ajay Gupta 2 , Kamalpreet Chhina 3 , Deepak Grover 4
1 Professor Department of Prosthodontics - D.J. College of Dental Sciences and Research, Modinagar
2 Head and Professor Department of Prosthodontics - D.J. College of Dental Sciences and Research, Modinagar
3 Professor & HOD) Department of Periodontology and Implantology - BRS Dental College and Hospital, Panchkula
4 Post Graduate Student Department of Periodontics - D.J. College of Dental Sciences and Research, Modinagar
|
| Address For Correspondence |
Dr. Bhawana Tiwari,
Professor Department of Prosthodontics (D.J. College of Dental Sciences and Research, Modinagar) |
| Abstract |
| ABSTRACT
The bilateral ankylosis of the temporomandibular joint is treated surgically; the procedure adopted involves reshaping of the ankylosed bony chunk using a 1.5 mm fissure bur. The cavity thus created is then either lined with dermis or silastic implant is placed to avoid fibrous reunion resulting due to contact of the newly created raw surfaces. Post operatively, the mouth opening in such patient is around 0.5 to 1.0 cm which is gradually made to increase to 3.0 to 4.5 cm by the use of stent as passive jaw exerciser given to maintain the surgically created mouth opening which is subsequently replaced by the dynamic jaw excerciser which the patient has to wear for atleast 18 hours a day.
The existing conventional jaw excerciser has 2 long beaks attached anteriorly to both the jaws as shown and is a cumbersome appliance and hence has low acceptability to the patient leading to reunion/ and ankylosis of the joint, hence the need to modify the appliance was undertaken. The newly devised dynamic jaw excersiser acts mainly on the posterior segment of the jaws and is more esthetically design resulting in better acceptability, appreciation, and improved compliance of the patient. |
|
| Keywords |
| Passive jaw excerciser, bilateral joint ankylosis, dynamic jaw excerciser, posterior segment, acceptability, stent, increased mouth opening |
|
| Full Text |
INTRODUCTION:
A method of exercise utilizing a jaw exercise device specifically configured to exercise the muscles of mastication including the temporal, masseter, external pterygoid and internal pterygoid[1].
The temporomandibular joint serves as a hinge for the lower jaw. The TM joint may become misaligned because of ankylosis, aging, arthritis, a blow to the jaw or head or yawning for prolonged periods with the mouth open too wide. Among the more common temporomandibular joint dysfunction symptoms are: earaches, tinnitus (ringing, tinkling, hissing), clicking, (Articular Crepitus), difficulty in opening the mouth (Trismus), headaches (particularly in the infratemporal region) and vertigo[2].
Most of the times muscle fatigue and spasm is present which is relieved with drugs like muscle relaxants and in post operative cases the use of TMJ excerciser is recommended [3].
MATERIAL AND METHODS:
The present invention relates to a method of jaw exercise utilizing a jaw exerciser device specifically configured to exercise the muscles of mastication. The conventional appliance has 2 acrylic plates, attached to maxillary and mandibular ridges/teeth having 2 beaks attached anteriorly which are made to connect with an elastic band. Once in position, the user exercises or uses the jaw exerciser device by consciously moving or opening his/her jaw against the elastic resistance force of the elastic bands. By repetitive exercise and use, the user or patient may strengthen the muscles of mastication. But this is a cumbersome appliance and hence has low acceptability to the patient.
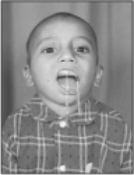
The newly devised dynamic jaw excersicer acts mainly on the posterior segment of the jaws. Impressions of the upper and the lower jaws are made with irreversible hydrocolloid material like alginate and acrylic plates are fabricated which are joined anteriorly. These plates mainly cover the posterior segments of the jaws. The patient can close or bite gently on the plates and the plates shall remain in a stable position. The elastic bands will keep the jaws open and the fatigue will force the patient to close the jaw against resistance. This will exercise the muscles and allow TM joint functioning (Fig.1). The basic purpose of the excerciser is to increase the opening of the mouth by moving of the jaws apart.
The conventional jaw excerciser makes the patient to exercise when the patient intentionally and forcibly closes the mouth. The jaws are pulled apart by reversal of elastic traction.
But in the newly deviced appliance, the traction created by the elastic bands results in automatic widening/ opening of the jaws. This action is passive resulting in prolonged opening of the muscles and the patient is forced to close the mouth against resistance (Fig.2).
This device is more esthetically designed resulting in better acceptability, more appreciation, and improves compliance of the patient.
DISCUSSION:
Mandibular hypomobility is a common sequela to many procedures performed by oral and maxillofacial surgeons.[4] This is especially true in the treatment of oral cancer in which rehabilitation after resection of the tumor is often complicated by fibromyositis
secondary to radiation therapy. [5] [6]Postoperative physical therapy is important to minimize mandibular hypomobility.[7]
One-piece jaw exerciser/strengthener, custom fit, aligned and retained on the teeth of the upper or lower jaws used to stimulate the jaw opening post operatively which is decreased as in cases of TMJ ankylosis (bilaterally) or bilateral fracture of the mandible at the condylar region, is used to stimulate the jaw opening and closing to avoid fibrous reunion of the joint post operatively.[8] The device is inexpensive, easy to use and has better acceptability with the patient.[9] Finally, because the opening force is controlled by the patients, they may believe that they are more in control of their treatment and may have less anxiety and increased compliance.[10] [11].
LEGENDS (PHOTOGRAPHS)
 | Increased mouth opening by moving the jaws apart
 |
 | Increased mouth opening by forcing to close the mouth against resistance
|
REFERENCES:
1. Darveniza M, Chapman PJ.A jaw exerciser for fibrous ankylosis of the temporomandibular joint. Australian Dental Journal, 1985 Dec; 30(6): 418-22.
2. Ross, John H. Jaw exercise device. United States Patent 4650182.
3. Gage JP. Jaw exerciser for fibrous ankylosis Aust Dent J. 1986 Jun;31(3):229-230.
4. Uriell P, Bertolucce L, Swaffer C: Physical therapy in the postoperative management of temporomandibular joint arthroscopic surgery. J Craniomandib Disorders 7:27, 1989
5.Rocabado M: Physical therapy for the post surgical TMJ patient. J Craniomandib Disorders 2:75, 1989
6.Hoffman D, Mannheimer J, Attanasio R, et al:
Management of the temporomandibular joint surgical patient. Clin Prevent Dent 11:28, 1989
7.Zislis MW, Wand HA, Gottehrer NR: TMJ arthroscopy-A preoperative and postoperative rehabilitation protocol. J Craniomandib Disorders 3:218, 1989
8.Bell WH, Gonyea W, Finn RA, et al: Muscular rehabilitation after orthognathic surgery. J Oral Surg 56:229,1983
9.Poremba EP, Moffett BC: The effects of continuous passive motion on the temporomandibular joint after surgery. Oral Surg Oral Med Oral Path 67:490, 1989
10.Storum KA, Bell WH: The effect of physical rehabilitation on mandibular function after ramus osteotomies. J Oral Maxillofac Surg 44:94, 1986
11Braun LB: The effect of physical therapy intervention on incisal opening after temporomandibular joint surgery. Oral Surg Oral Med Oral Path 64:544, 1987. |
|
|
|
|
|
|