Introduction
Endodontic treatment encompasses procedures that are designed to maintain the health and integrity of all or part of the pulp. When the pulp is diseased or injured, treatment is aimed at preserving normal periradicular tissues. When pulpal disorders spread to the periradicular tissues, treatment is aimed at restoring them to health. This is usually achieved by root canal treatment.
The term “root canal” has become fashionable and generally known. In conversation, people proudly proclaim that they have had a “root canal.” The stigma of fear and pain is fast disappearing. There is no question that the public’s acceptance of endodontic treatment is on the rise. In 1969, the American Dental Association (ADA) estimated that 6 million root canal fillings were done each year.[1] Root canal treatment is considered an essential element in the dental services provided to the population in developed countries.
Many surveys by different researchers were carried out to investigate the standard of root canal treatment carried out by dental practitioners in European countries.[2],[3],[4] Researchers also observed and concluded that dental colleges and schools were responsible in indoctrinating standard guidelines related to root canal therapy.[5],[6] Several studies have revealed that the majority of dentists do not comply with the formulated guidelines on the quality of root canal treatment.[2],[3],[4],[7] Studies have also shown the attitude of dentists in Western countries such as Germany,[2] UK,[3] Belgium [4] and USA.[7] The greatest share of endodontic procedures is carried out by America’s general practitioners. The specialty of endodontics is growing. In 1986, only 5% of those patients who had root canal therapy were treated by a specialist. By 1990, this percentage had grown to 28.5%. In 1989, there were 2,500 endodontic specialists in the United States. By 2,000, the figure was around 3,300 endodontists, and these endodontists were completing 39% of all of the root canal therapy and endodontic surgery in the United States.[1] The fact that general dentists do more endodontic cases than specialists has greatly affected the treatment outcome. Though many surveys tell the general endodontic practice protocol in developed nations [2], [3],[4],[6] few studies have however investigated the attitude of general dental practitioners toward various aspects of endodontic treatment in developing countries.[8][9][10]
The aim of this survey was to ascertain the endodontic practice protocol among a subpopulation of Indian Dentists.
Material & Methods
A questionnaire was given to 150 general dental practitioners in Uttar Pradesh to investigate common materials and techniques employed in root canal treatment. The questionnaire consisted of questions concerning different aspects of endodontic treatment including root canal therapy stages, materials, the choice of instruments, the use of various isolation methods, the use of canal irrigants, the use of intracanal medicaments and the choice ofobturation technique. A self-administered questionnaire was used to assess the main outcomes of the study. Questionnaire items were carefully selected from relevant published reports in international journals.[3],[4], [6],[7]
The collected data was analyzed using the statistical package SPSS. Simple descriptive statistics were used together with Chi-square (χ2) test. The chosen level of significance was set at P < 0.05. Unanswered questions were treated as missing values.
Results
Of the 150 questionnaires distributed (n=150), 131 completed replies were received, which is 87.3% response rate. All the respondents performed endodontic treatment including molar endodontics.
The distribution of the respondents according to the years of professional experience is shown in Table 1. Years in practice were not evenly distributed amongst the total respondents. The number of the first two groups (0–5 and 6–10) consisted of more than half the total respondents due to the significant increase in the number of graduates in the last 10 years. 82% of the respondents were males, 18% were females.
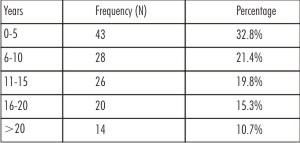 | Table 1: Professional Experience Of The Respondents
 |
Table 2 shows that combination of cotton rolls and high volume suction (36.64%) is the most commonly used method for moisture control followed by cotton rolls (34.35%) and high volume suction separately (22.9%). Rubber dam is least used for isolation (1.5%).
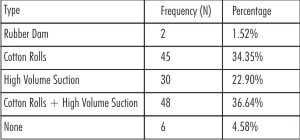 | Table 2: Methods Of Isolation Used By Respondents
|
Table 3 shows the hand instruments used for preparationof the root canal. K-files were the most popular instruments. More than half of the respondents utilized K- files solely for the preparation of root canal. Filling or push pull technique was the most popular technique for the preparation of root canal. Almost 53 % of the respondents utilized filling technique. Step back and step down were advocated by 27.5% and 19.8% respondents respectively as shown in Table 4.
 | Table 3: Root Canal Instruments Used By Respondents
|
 | Table 4: Root Canal Preparation Technique Employed By Respondents
|
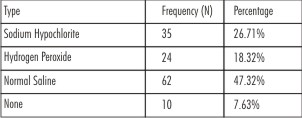
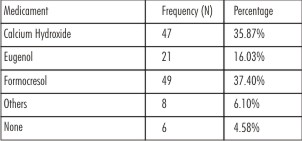
Disinfection, the most critical step of endodontic therapy often goes neglected. Tables 5 and 6 show the popular materials used in root canal disinfection and their frequency of use. Practitioners who were the part of this survey advocated normal saline (47.32%) and sodium hypochlorite (26.71%) as the most frequently used root canal irrigants. Formocresol was the most preferred intracanal medicament. Calcium hydroxide was routinely used by 35% of the respondents while 4.58% participants did not use any medicament at all.
 | Table 5: Irrigants Used By Respondents
|
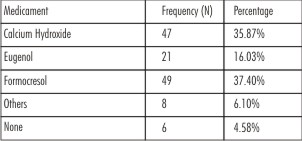 | Table 6: Intracanal Medicaments Used By Respondents
|
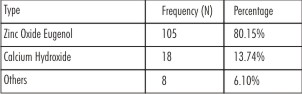
Tables 7 and 8 highlight the type of materials and techniques used in obturation of radicular space. From the results it was found that Zinc oxide eugenol (80.15%) and lateral condensation technique (61.83%) were most frequently used.
 | Table 7: Type Of Sealers Used By Respondents
|
 | Table 8: Obturation Technique Employed By Respondents
|
Discussion
This survey was conducted with an aim to assess the practice protocol adopted by general practioners in an Indian subpopulation.The response rate was 87.3% which was higher than in many previous surveys conducted in Western countries with better communication infrastructure.[3],[8],[11],[12] The results of this study revealed several interesting patterns of knowledge and opinions among the participating oral health care professionals regarding the materials and techniques used during the course of endodontic treatment.
A questionnaire was sent to general dental practitioners using e-mail. The distribution of the survey via e-mail and collection of data via an online interface offer a unique set of strengths and weaknesses. This method facilitates access to large groups at a relatively low cost, improves response percentages by offering the ability to send reminder e-mails and guarantees completion of each question by using an incomplete error message for unanswered questions during the submission process. On the other hand, the online interface has a risk of introducing bias into the survey by excluding dentists without e-mail addresses. Potentially, these dentists might be more resistant to adopting new technologies or less likely to interact with their peers as a result of fewer avenues of communication.
Results of this survey proved that majority of participants have comparatively lesser practicing experience. This can be attributed to the fact that more dental institutions have come up resulting in significant increase in the number of graduates in the last 10 years.
Isolation of the operating field plays an important role in patient and doctors protection by avoiding aspiration or swallowing of small instrument and debris. Improving the access and visibility of the operating field by moisture control, gingiva, lips and cheek retraction hence improving the operating efficiency and the properties of the restorative materials used, thus leading to better results
Application of rubber dam is always recommended as a standard during root canal treatment procedure to provide isolation, protection and improve visual access. In our survey only two (1.5%) dentists reported using rubber dam very occasionally and not as a routine practice. The results were consistent to the ones which were conducted amongst Sudanese (2%) and Flemish dentists (3.4%).[7],[9] But surveys conducted amongst American and British dentists emphasized the routine usage of rubber dam for isolation. 59% of American dentists,[7] 60% of dentists in UK[13] and 57% of general dental practitioners in New Zealand [14] reported using rubber dam routinely in endodontic treatment. Koshy et al[14] cited extra cost, additional time, lack of adequate skills or training, absence of patient's acceptability or inadequate education in the undergraduate teaching curriculum as the potential reason for less use of rubber dam. Results from the present survey proved that the respondents preferred cotton rolls and high volume suction as a method for moisture control and isolation. This can be due to its cost effectiveness and ease of use.
Biomechanical preparation is a critical step in success of endodontic therapy.Along with diligent access preparation, canal location and working length determination only thorough biomechanical preparation will ensure good obturation and healing.[15] Results from present investigations showed that K- File was the preferred instrument by more than half of the respondents (57.2%) while 22.9% respondents preferred using Files and reamers.The push pull technique (filing) was the most popular canal preparation technique among the participating general dental practitioners (52.7%). These results were in agreement with Hommez et al[16] who concluded that 60.4% of Flemish dentists used the standard filing technique. Respondent dentists tended to use hand instruments and were not inclined to use more advanced engine driven techniques for shaping the root canal system.
One of the most neglected phases of endodontic treatment is the removal of minute fragments of organic debris and dentinal shavings from the root canal. A principle of surgery is that before a wound is ready for disinfection;all the necrotic materials and debris must be removed. Many dentists fail to appreciate the importance of this basic rule of surgery and rely principally on drug therapy rather than thorough cleaning and irrigation of the root canal. Proper cleaning and debridement are as necessary in endodontic treatment as in surgery. Following thorough instrumentation of an infected root canal there will be a significantly reduced number of bacteria present, but it is well documented that instrumentation alone cannot clean all the internal surfaces of the root canal. Bacteria can be found on the root canal walls, within dentine tubules and in lateral canals. Antibacterial irrigants and interappointment medicaments are needed to kill the remaining micro-organisms.[17] Cleaning and shaping are the most important factors in the endodontic procedure, and intracanal medication dressing of the root canal is secondary in root canal treatment.[18]
47.3% of the respondents participating in the survey used normal saline as the principal irrigant while 26.7% used sodium hypochlorite as the primary irrigant. 7.6% dentists participating did not use any irrigant. These results were in disagreement to the survey conducted by Barbakow[12] who propagated the use of sodium hypochlorite. However Siqueira et al[19] in their study concluded that when normal saline was used in irrigation and the size of apical preparation was increased from #30 to #40, there was a significant reduction in number of bacteria. Less use of sodium hypochlorite might be attributed to the fact that only 1% of the participants used rubber dam for moisture control.
According to a study by Bystrom and Sundqvist,[20] when no intracanal medication was used between appointments, pathogenic microorganisms increased in number. Thus, they recommended the use of an intracanal medication dressing between appointments. Despite the fact that calcium hydroxide is recognized as the standard intracanal medicament for inter-appointment dressing, [21] it was used by only 35.8% of the respondents. Majority of the general practitioners reported using formaldehyde-containing materials. This finding is consistent with previous findings recorded for Sudanese dentists.[10] Although formaldehyde- containing products have been used for their antimicrobial and fixative properties, they are toxic to periradicular tissues[22] and may have mutagenic and carcinogenic potential.[23] The use of calcium hydroxide, as intracanal medication, should be encouraged as it is effective against most root canal pathogens and able to denature bacterial endotoxins.[24],[25] It has, also been reported to be the material of choice by dentists in the Western countries.[12],[26]
The hermetic sealing of the root canal system is in an important phase of the root canal treatment.[27],[28] Almost 61% of the respondents used cold lateral compaction of gutta-percha to obturate the root canal space. This technique is acknowledged universally and is the most common obturation technique.[5] Zinc oxide eugenol was the sealer of choice and was used by more than 80% of the participants. This can be due to the fact that it is easily available, cost effective and easy to manipulate. Seemingly, the respondents were not strong advocates of the more recently introduced advanced obturation techniques. This may be attributed to additional cost involved or the lack of skill and training.
Conclusion
Root canal treatment usually fails when treatment falls short of acceptable standards. This study investigated the status of endodontic practice among general dental practitioners in Uttar Pradesh. The results of questionnaire survey indicated that differences between daily general practice and academic teaching exist. The results the present study indicated that majority of general practitioners disregard the most basic principles of endodontic treatment. It demonstrated that dentists performed procedures which often deviated from well acknowledged endodontic quality guidelines. Dentists did not use rubber dam for isolation and frequently use formaldehyde-containing materials for inter-appointments dressing. The most striking finding was the generally negative attitude amongst general dental practitioners towards performing endodontic treatment and adoption of new technologies in a daily endodontic practice and relied on old conventional methods.
It might be also concluded that root canal treatment is technically demanding and is often in general practice carried out under less than optimal conditions. This survey shows the importance of establishing higher specialist training or continuing dental education for practitioners to update their knowledge.
References
1. Ingle JI, Harold SC (2002) Ingles Endodontics. 5thed, BC Decker Inc, London, 1-35.
2. Weiger R, Hitzler S, Hermle G, Löst C. Periapical status, quality of root canal fillings and estimated endodontic treatment needs in an urban German population. Endod Dent Traumatol 1997; 13: 69-74.
3. Jenkins SM, Hayes SJ, Dummer PM. A study of endodontic treatment carried out in dental practice within the UK. Int Endod J 2001; 34: 16-22.
4. Slaus G, Bottengerg P. A survey of endodontic practice amongst Flemish dentists. Int Endod J 2002; 35: 759-767.
5. Qualtrough AJ, Whitworih JM, Dummer PM. Preclinical endodontology: an international comparison. Int Endod J 1999; 32:406-414.
6. European Society of Endodontology. Consensus report of the European Society of Endodonology on quality guidelines for endodontic treatment. Int Endod J 1994; 27: 115-124.
7. Whitten BH, Gardiner DL, Jeansonne BG, Lemon RR. Current trends in endodontic treatment: report of a national survey. J Am Dent Assoc 1996; 127: 133-341.
8. Akpata ES. Endodontic treatment in Nigeria. Int Endod J 1984; 17: 139-151.
9. Maina SW, Ng'ang'a PM. Root canal treatment and pulpotomy in Kenya. East Afr Med J 1991; 68: 243-248.
10. Ahmed MF, Elseed Al, lbrahim YE. Root canal treatment in general practice in Sudan. Int Endod J 2000; 33: 316-319.
11. Pitt Ford TR, Stock CJ, Loxley HC, Watsson RM. A survey of endodontics in general practice in England. Br Dent J 1983; 83: 222-224.
12. Barbakow F. The status of root canal therapy in Switzerland in 1993. J Dent Assoc S Afr 1996; 51: 819-822.
13. Whitworth JM, Seccombe GV, Shoker K, Steele JG . Use of rubber dam and irrigant selection in UK general dental practice. Int Endod J 2000; 33: 435-441.
14. Koshy S, Chandler NP. Use of rubber dam and its association with other endodontic procedures in New Zealand. N Z Dent J 2002;98: 12-16.
15. Cohen S, Burns RC (1991) Pathways of the pulp. 5th ed, Times Mirror/Mosby College Publishing, St. Louis, 77-110.
16. Hommez GM, Braem M, De Moor RI. Root canal treatment performed by Flemish dentists. Part I. Cleaning and shaping. Int Endod J 2003; 36: 166-173.
17. Grossman LI, Oliet S, Del Rio CE (1988) Endodontic practice. 1lth ed, Lea &FebigerInc, Philadelphia, 228-233.
18. Itoh A. A Survey of Filling Methods, Intracanal Medications and Instrument Breakage. J Endod 1999; 25: 823-824.
19. Siqueira JF, Lima KC, Magalhaes FA. Mechanical reduction of bacterial population in root canal by three instrumentation technique. J Endod 1999; 25: 332-335.
20. Bystrom A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J 1985; 18: 35-40.
21. Chong BS, Pitt Ford TR. The role of intracanal medication in root canal treatment. Int Endod J 1992; 25: 97-106.
22. Gulabivala K (1995) lntracanal medication and temporary seal. In: Color Atlas and Text of Endodontics 1995, 2nd ed, Mosby-Wolfe,145-150.
23. Spangberg I (1994) Intracanal medication. In: Endodontics, 4th ed, Williams and Wilkins, USA, 627-640.
24. Bystrom A, Claesson R, Sundqvist G. The antibacterial effect of camphorated paramonochlorphenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent Traumatol 1985;1: 170-175.
25. Sjögren U, Figdor D, Spangberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J 1991; 24: 119-125.
26. Hommez GM, Braem M, De Moor RJ. Root canal treatment performed by Flemish dentists. Part 2. Canal filling and decision for referrals and treatment of apical periodontitis. Int Endod J 2003; 36: 344-351.
27. Schilder H. Filling root canals in three dimensions. J Endod 2006; 32: 281–290.
28. Goodis HE. Commentary on: filling root canals in three dimensions. J Endod 2006; 32: 279–280.
|