Introduction
Dentists experience more lower back pain than do practitioners in other occupational groups[2]. A study of back pain in dentistry (2005) concluded that 86 % of dentists in Glasgow reported back pain at some point in their career thus indicating the severity of the problem. 83% of these dentists believe this pain was due to posture at work.
Dentist could be at ergonomic risk, depending on the number and type of procedure they perform, the position that they occupy during a procedure and the extensiveness of the procedure itself[1].
Cumulative trauma disorders (CTD) is defined as musculoskeletal disorders that can result from the body's inability to heal itself from the long-term effects of repetitive motion, exposure to vibration, and/or mechanical stress. It is a syndrome that affects muscles, tendons, nerves and blood vessels. It commonly involves the hands, arms and upper back. Lower limbs may also be affected[5].
Dental health-care personnel (DHCP) are most prone to CTD’s as they commonly assume awkward work postures to obtain better intraoral view, provide a more comfortable position for the patient. Dentists, moreover, coordinate their position relative to the patient or assistant and inadvertently achieve uncomfortable postures while reaching for instruments and supplies.
Contributing factors
-
Routine exposure to:
-
Forceful hand exertions
-
Grasping small instruments for prolonged periods
-
Forceful squeezing/release of instruments
-
Repetitive movements
-
Fixed or awkward postures
-
Vibrating tools
-
Unassisted frequent or heavy lifting
Risk factors
Associated with dentistry:
-
Prolonged static neck flexion
-
Shoulder abduction or flexion
-
Lack of upper-extremity support
-
Inadequate work breaks
Signs and symptoms of most commonly seen CTDs
1. Myofascial Pain Disorder[8]
Pain and tenderness in the neck, shoulder, arm muscles
Painful trigger points - may twitch upon touch or massage
Restricted range of motion
Possible causes: overloaded neck/shoulder muscles
2. Cervical Spondylosis[11]
Intermittent/chronic neck and shoulder pain or stiffness
Headache
Hand and arm pain, numbness, tingling, clumsiness may occur
Possible causes: age-related spinal disc degeneration leading to nerve compression and spinal cord damage; arthritis
3. Herniated Spinal Disc
Back and leg numbness, tingling, pain, weakness
Worsens with coughing, sneezing, sitting, driving, bending forward
Possible causes: bulging or fragmenting of intervertebral discs into spinal canal compressing and irritating spinal nerves; excessive heavy lifting without adequate rest
4. Lower Back Pain[9]
Low back pain was found to be the most prevalent musculoskeletal complaint, reported by 46% of the dentists[3]. Pain
Stiffness in lower spine and surrounding tissues
Possible causes: heavy lifting and forceful movements; whole body vibration;bending/twisting; awkward static postures
5. Sciatica[10]
Pain from lower back or hip radiating to the buttocks and legs
Leg weakness, numbness, or tingling
Possible causes: prolapsed intervertebral disc pressuring the sciatic nerve; worsened with prolonged sitting or excessive bending/lifting
6. Carpal Tunnel Syndrome[6],[7]
Pain or tingling that awakens the patient at night with relief via shaking/massaging the hand is considered a hallmark symptom for diagnosis
Eventual muscle weakness and atrophy
Symptoms often worse with increased activity
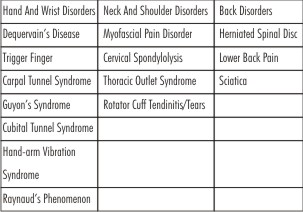 | Cumulative traumatic disorders (CTD) affecting dentists can be broadly classified into:
 |
Ergonomics
Ergonomics is the science of fitting workplace conditions and job demands to the capabilities of employees. A practical approach to Ergonomics considers the match between the person, the equipment they use, the work processes and the work environment. A persons capabilities, physical attributes and work habits must be recognized to improve ergonomic factors in the workplace[12].
Applying Ergonomics to Dentistry
While setting up the dental practice, following suggestions should be kept in mind:
1. Provide sufficient space
Permanently place equipment used in every clinical procedure within comfortable reach (within 20 inches of the front of the body). Use mobile carts for less commonly used equipment to allow convenient positioning when required.
2. Accommodate individual needs and preferences
Individuals vary in size, shape, training, and experience. Ensure that equipment and work areas allow flexibility for examples
-
Allow right- or left-handed use
-
Allow different working postures
-
Provide a choice in methods used
3. Reduce physical effort
All effort should be made to avoid bent or unnatural postures. Ideally, equipment should allow work in a relaxed and well-balanced position
4. Instrument selection
The goal of proper instrument selection should be to reduce force exertion and maintain hand/wrist in neutral position with no wrist bend. Always consider the overall shape/size, handle shape/size, weight, balance, maneuverability and ease of operation and maintenance of the instrument.
5. Magnification
Latest advancements in dentistry like operating microscopes and loupes if used correctly can be a boon to the dentist. The aim should be to improve neck posture and provide clearer vision. Loupes used by dentists help to magnify objects allowing easier detection of things that are difficult to see e.g. root canals and cavity margins. They also act to enhance posture as the dentist can sit more upright and not have to be as close to the patient as possible to accurately view the treatment they are carrying out[4]. While selecting the magnification systems consider
-
Working distance
-
Depth of field
-
Declination angle
-
Convergence angle
-
Magnification factor
-
Lighting needs
6. Operator Chair
A good seating position and correct posture is vital for the efficient practise of dentistry and to avoid chronic back pain[2]. An ideal operator stool should promote mobility and patient access as well as accommodate different body sizes. While selecting the dentist should look for:
-
Stability
-
Lumbar support
-
Hands-free seat
-
height adjustment
7. Scheduling
The dental surgeon should be careful to schedule appointments to provide sufficient recovery time and avoid muscular fatigue. Some suggestions in this regard are:
-
Increase treatment time for more difficult patients
-
Alternate heavy and light calculus patients within a schedule
-
Vary procedures within the same appointment
-
Shorten patient’s recall interval
Conclusion
Dentist should maintain the shape of the spine in a natural ‘S-shape’ rather than strained seating position therefore creating an upright posture. The pelvis should be correctly positioned during work so that less stress is placed on the spine i.e. its curvature is controlled. All the years of training, skill acquisition, and capital investment are worth nothing if you can't hold up to the physical demands of dental practice and then retire healthfully.
References
1. James B. Bramson. Evaluating Dental Office Ergonomics. Risk Factors and Hazards. JADA ; 1998: 174-183
2. David W. DMD et al. Reports of body pain in a dental student population. JADA ; 2005: 81-86.
3. Alexopouios, Evangelos C. et al. Prevalence of musculoskeletal disorders in dentists. Musculoskeletal Disorders; 2004: 5:16
4. Christensen GJ. ‘Magnification in dentistry: useful tool or another gimmick?’ JADA 2003 Dec 134 (12) 1647-50
5. Al-Otaibi T. Repetitive Strain Injury. Saudi Med J 2001 ; 22 : 398-402.
6. Wilkins r, rengachary s. neurosurgery. 2nd edn. McGrawhill : 3074 – 3078.
7. Bradley w. neurology in clinical practice. 5th edn. 425 – 431.
8. Bradley w. neurology in clinical practice. 5th edn. 431 – 433.
9. Bradley w. neurology in clinical practice. 5th edn. 441 – 445.
10. Youman. Neurological surgery. 5th edn. 4507 – 4511.
11. Ramamurthy b, tandan p. textbook of neurosurgery. 2nd edn. 775 – 777.
12. Nutalapati r, gaddipati r et al. ergonomics in dentistry and the prevention of musculoskeletal disorders in dentists. The internet j of occupational health; 2010 : 1.
|