Introduction:
An ‘open apex’ is the presence of an exceptionally wide root canal at the apex and occurs when root development ceases as a result of pulpal necrosis in newly erupted teeth which may be due to trauma, extensive apical resorption, root-end resection or over-instrumentation.
Treatment of such teeth pose many challenges including increased risk of root fracture, difficulty in canal length determination, difficulty in instrumentation and obturation of the wide, apically divergent and thin canals [1], [2], [3]. An accurate working length results in effective cleaning and shaping procedures confined within the root canal system and paves the way for a fluid tight obturation of all the portals of exit thus ensuring long term success of the treated tooth. Traditional methods of root canal length estimation like radiographs, apex locators and paper point evaluation are usually inadequate in such situations. This case report elicits the use of “Tactile Method” for accurate working length measurement in a maxillary anterior tooth as suggested in a previously published invitro study [4].
Case Report
A 21 years old female patient reported to the author’s clinic with a chief complaint of pain and discoloration with tooth no 21. Patient gave a childhood history of trauma to her front tooth and was found to be a mouth breather.
On clinical examination, the tooth in question was mildly painful on vertical percussion and discolored with an Ellis Class II fracture mesially [Fig. 1].
 | Fig. 1: Pre-operative photo showing fractured and discolored 21.
 |
An intraoral periapical (IOPA) radiograph of the tooth revealed presence of an open apex, and diffuse periapical radiolucency [Fig. 2].
 | Fig. 2: IOPA of the tooth showing large open apex and a diffuse periapical radiolucency.
|
The tooth was nonresponsive to heat testing. A diagnosis of pulpal necrosis associated with periapical pathology & large open apices with tooth no. 21 was made. After discussing various treatment options, the patient agreed to a treatment plan consisting of root canal treatment without rubber dam application (as the patient was a mouth breather and rejected the use of rubber dam vehemently), orthograde apical Mineral Trioxide Aggregate(MTA) plug and gutta percha obturation.
After securing local anesthesia to ease the mild painful symptoms, and access opening and pulpectomy, a size 120 H file (Dentsply Maillefer, France) was introduced till the estimated length (as measured from the preoperative IOPA) and found to be loose [Fig. 3]. Due to paucity of time an Intra Canal Medicament (ICM) of calcium hydroxide with iodine (Metapex, Meta Biomed Co, Korea) was placed in the canal, the tooth temporized with Zinc oxide eugenol (ZOE) temporary filling. The patient was prescribed Nonsteroidal Anti Inflammatory Drugs (NSAIDs) asked to report the next day for further treatment. Antibiotics were not prescribed as the patient was afebrile and did show any signs of regional lymphadenopathy.
 | Fig. 3: IOPA showing no.120 H file loose at apex with 21.
|
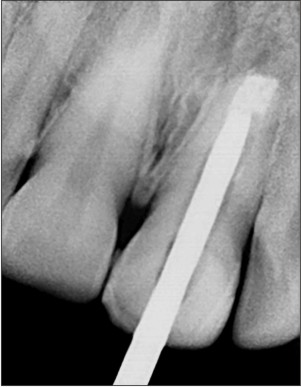
The next day the “The Tactile Method” for estimating the canal length as suggested by ElAyouti A. et al was used [4]. After removing the temporary filling and the ICM, a size 25 (2% taper) stainless steel hand K file (Dentsply Maillefer, France) was bent at an angle of 90o at the tip (~1mm) using a universal orthodontic plier. The rubber stopper of the file was adjusted to a length as judged from the preoperative radiograph. The “Tactile Working Length” (TWL) for the root canal was determined by inserting the bent file into the canal and moving it apically along the root dentinal wall until it engaged the lip of the dentin at the apex [Fig. 4]. Care was taken not to injure the periapical tissues by over insertion. The silicon stopper was adjusted to a reference point at this length and the file disengaged from the root by turning it a full 90o, withdrawn and measured. Measurements were made with the bent portion facing mesial, distal, buccal and palatal and the length recorded as 19.6mm, 19.5mm, 19mm and 19mm respectively. The lowest figure of 19mm was taken as the TWL of the tooth.
 | Fig. 4: Bent no. 25 K file and schematic diagram of “The Tactile Method”
|
Digital intraoral periapical xrays (Kodak RVG 5000) of mesial & distal measurements were taken for record keeping [Fig. 5, 6].
 | Fig. 5: IOPA showing the bent no. 25 K file engaging the mesial lip of the root apex (radiopaque ICM also visible at the apex).
|
 | Fig. 6: IOPA showing the bent no. 25 K file engaging the distal lip of the root apex (radiopaque ICM also visible at the apex).
|
The canal was then cleaned and shaped with size 120(2% taper) K file (Dentsply Maillefer, France) using gentle circumferential filing of the dentinal walls and irrigated carefully using 3% sodium hypochlorite and 0.9% w/v saline alternatively. The canals were dried with paper points and the ICM was replaced in the canals and tooth temporized with ZOE. The patient was discharged and recalled after 10 days for evaluation.
The patient returned for recall after 3weeks, the temporary filling was removed and the canal was irrigated with copious saline to remove the ICM. The canal was dried with paper points and an apical plug of MTA (ProRoot MTA, Dentsply Tulsa, USA) was introduced in the apical 3mm following the manufacturer’s instructions, a moist cotton pellet was then placed inside the canal, the tooth temporized and patient discharged.
After 24hrs the tooth was reopened and the MTA plug was probed with a smooth broach to confirm that it had set [Fig. 7]. The tooth was then obturated using chemically plasticized roll cone gutta percha using 1min chloroform (Bipin Enterprises, India) dip [Fig. 8, 9]. The patient was discharged and told to report after 2-3 weeks.
 | Fig. 7: IOPA showing MTA plug in apical 3mm.
|
 | Fig. 8: IOPA showing gutta percha master cone.
|
 | Fig. 9: IOPA showing obturated tooth.
|
After two weeks core buildup was done using dual cure composite resin, the tooth was then restored to form, function and esthetics with a full coverage ceramic crown [Fig. 10].
 | Fig. 10: Full coverage ceramic crown with 21.
|
The patient was recalled after one year and the tooth was found to be normal to percussion tests, a radiograph was also taken to ascertain adequate periapical healing [Fig. 11].
 | Fig. 11: IOPA taken after one year showing adequate periapical healing with 21.
|
Discussion:
An accurate working length is essential for preventing overinstrumentation and overfilling and attaining optimum success during root canal treatment [5],[6].
In teeth with open apices the radiographic interpretation of canal length is even more difficult due to the altered apical anatomy and the missing periodontal ligament space at the apex [7],[8]. Apex locators are of little use in such situations, asthe wide root canals associated with open apices, adversely influence the function of apex locators [9],[10],[11],[12].
Paper point technique may be used in such cases. This technique requires the canal to be completely dry and the periapical tissues to be relatively moist. In open apices, the control of moisture is difficult because the contact area to the inflamed periapical tissues is large, and excess moisture is common, which may result in measurement errors.
Moreover, to obtain accurate measurements when using paper points, the periapical tissues must be located at the same level of the apical terminus, a condition that may not be fulfilled in open apices, (because of down growth of periapical tissues into the canal up to a distance of 3 mm) which may result in short measurements [13].
The invitro accuracy of “The Tactile Method” was 97.7% within a range of ±0.5mm. This method is however not feasible in curved canals or in teeth with an apical size smaller than no. 100 as the gauging instrument needs to be dragged along the canal wall and twisted once beyond the apex with the bend being 1mm coronal to the tip of the instrument [4].
The size of the file used in this case was no 25(2% taper); this provided enough instrument stiffness to probe the dentinal wall; a larger size may be used if the situation permits.
The difficulty one experiences in disengaging of the file tip from dentinal wall can be overcome by curving the file along the shaft and slightly rotating it on removal out of the canal. The operator’s orientation may be further enhanced by adjusting the marker on the silicon ring to indicate the direction of the bent tip. One needs to work very cautiously while inserting and hooking the file (when at the apex); as there are chances of injuring the periapical tissues which will impede adequate healing. Practising on simulated canals is highly recommended.
Conclusion
Open Apices are difficult cases to manage. In straight canals part of the problem associated with inaccurate working lengths may be solved if one uses “The Tactile Method” presented in this clinical report. However the use of this technique is limited only to canals larger than file size 100 and should not be tried in curved canals.
References:
1. Allen R, Mackie IC. Management of the immature apex - a clinical guide. Dent Update 2003; 30(8):437–41.
2. Dominguez Reyes A, Munoz Munoz L, Aznar Martin T. Study of calcium hydroxide apexification in 26 young permanent incisors. Dent Traumatol. 2005; 21(3):141-5.
3. Bogen G, Kuttler S. Mineral trioxide aggregate obturation: a review and case series. J Endod. 2009; 35(6):777-90.
4. ElAyouti A, Dima E., Lost C. A tactile method for canal length determination in teeth with open apices. Int Endod J.2009; 42(12):1090-5.
5. Shabahang S, Torabinejad M, Boyne PP, Abedi H, McMillan P. A comparative study of root-end induction using osteogenic protein-1, calcium hydroxide, and mineral trioxide aggregate in dogs. J Endod.1999; 25(1):1-5.
6. Holland R, Mazuqueli L, de Souza V, Murata SS, Dezan Junior E, Suzuki P. Influence of the type of vehicle and limit of obturation on apical and periapical tissue response in dogs’ teeth after root canal filling with mineral trioxide aggregate.J Endod. 2007; 33(6):693-7
7. ElAyouti A, Weiger R, Lost C (2001) Frequency of overinstrumentation with an acceptable radiographic working length. J Endod.2001; 27(1):49–52.
8. Williams CB, Joyce AP, Roberts S. A comparison between in vivo radiographic working length determination and measurement after extraction. J Endod. 2006; 32(7):624-7.
9. Ebrahim AK, Wadachi R, Suda H. Ex vivo evaluation of the ability of four different electronic apex locators to determine the working length in teeth with various foramen diameters. Aust Dent J. 2006; 51(3):258-62.
10. Herrera M, Abalos C, Planas AJ, Llamas R. Influence of apical constriction diameter on root ZX apex locator precision. J Endod.2007; 33(8): 995–8.
11. Tosun G, Erdemir A, Eldeniz AU, Sermet U, Sener Y. Accuracy of two electronic apex locators in primary teeth with and without apical resorption: a laboratory study. Int Endod J.2008; 41(5):436–41.
12. Goldberg F, De Silvio AC, Manfre S, Nastri N. In vitro measurement accuracy of an electronic apex locator in teeth with simulated apical root resorption. J Endod. 2002; 28(6):461-3.
13. Rosenberg DB. The paper point technique, part 1. Dent Today. 2003; 22(2):80-6
|