Introduction
Amelogenesis imperfect is a condition we routinely encounter in our clinical practice
The degree of defect varies from patient , a severe presentation has a debilitating esthetic and functional impact on the patient. The following case report highlights the management of such a case.
Case Report
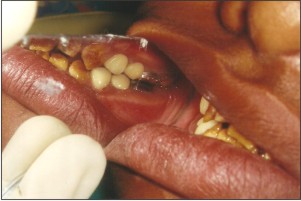
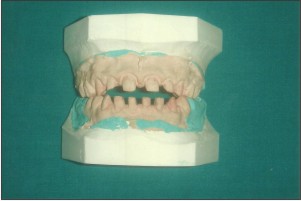
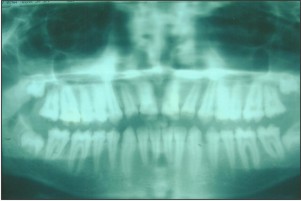
A 14yrs old male patient reported to the clinic with the complaint of inability to chew his food properly and also suffered from esthetic inadequacy and sensitivity of his teeth. He expressed extreme dissatisfaction with his appearance. A detailed medical and dental examination was performed including photographs and dental radiographs.(Fig 1,2,3)
 | Fig 1
 |
 | Fig 2
|
 | Fig 3
|
AmelogenesisImperfecta (AI) is an heterogenous genetic disorder that disturbs the developing enamel structure.[1] This rare ectodermal defect leads to a variety of clinical manifestations due to agenesis, hypoplasia, and/or hypomineralisation of the enamel.[2]
In the present case tissue loss affected all the teeth. Enamel had a mottled appearance with a yellow brown discoloration. The mottled enamel had the same radiodensity as dentin. It was concluded that the patient likely suffered from a hypomaturation type of AmelogenesisImperfecta.The family history reported no such evidence of such a condition.
Oral hygiene was not judged satisfactory at the first visit although the patient demonstrated a good knowledge of correct oral hygiene, this could be probably due to the sensitivity of teeth. A decreased occlusal vertical dimension was evident.
A treatment plan was developed with the main objectives to raise the vertical dimension of teeth, enhance the esthetics, restore masticatory function and eliminate the teeth sensitivity.[3]
The vertical dimension of the teeth was increased by 2mm by means of an acrylic splint for 3 weeks(Fig 4,5,6).
 | Fig 4
|
 | Fig 5
|
 | Fig 6
|
After opening of bite, maxillary and mandibular first molars were prepared for full crown restorations which were then restored with glass ionomer luting cement .(Fig 7,8,9)
 | Fig 7
|
 | Fig 8
|
 | Fig 9
|
Keeping in mind the smile line of the patient and functional requirements, maxillary and mandibular first and second premolars were prepared for porcelain fused to metal crown with porcelain facing.
Taking into consideration the thickness of teeth in anterior segment and the age of patient, elective root canal treatment was done for maxillary and mandibular anterior teeth followed by preparation of all ceramic crowns which were then cemented with resin cement.(Fig 10,11,12,13,14,15)
 | Fig 10
|
 | Fig 11
|
 | Fig 12
|
 | Fig 13
|
 | Fig 14
|
 | Fig 15
|
After the restorative procedures, dental hypersensitivity of the patient was reduced satisfactorily and satisfactory function and esthetics was established.
The patient was recalled after two months. The patient’s oral hygiene was satisfactory. The restorations remained with no discoloration, crazing or carious lesions. The patient's esthetic and functional expectations were satisfied.[4] (Fig 16)
 | Fig 16
|
Conclusion
With the above mentioned treatment, patient was treated not only from a functional and esthetic standpoint, but also from a psychosocial standpoint by upgrading his quality of life and helped in reinforcing his self-esteem.[5]
References
1. Functional and esthetic rehabilitation of a patient with amelogenesisimperfecta. Ergun G, Kaya BM, Egilmez F, Cekic-Nagas I. J Can Dent Assoc. 2013 May; 79:d38
2. Prosthodontic management of patients with amelogenesisimperfecta. Hoods-Moonsammy VJ, Mothopi MM, Taruvingira AK, Owen CP, Howes DG. SADJ ; 2012 Aug ; 67(7): 409-12
3. Functional and esthetic rehabilitation of mutilated dentition associated with amelogenesisimperfecta. Mete JJ, Dange SP, Khalika AN, Vaidya SP. J Indian Prosthodont Soc. 2012 Jun; 12(2) : 94-10
4. Oral rehabilitation of a patient with amelogenesisimperfecta. Cogulu D, Becerik S, Emingil G, Hart PS, Hart TC. Pediatr Dent 2009. Nov-Dec; 31(7) : 523-7
5. Amelogenesisimperfecta, hypoplastic type associated with some dental abnormalities: a case report. Canger EM, Celenk P, Yenísey M, Odyakmaz SZ. Braz Dent J. 2010; 21(2) : 170-4
|