Introduction
The main aim of Prosthodontic rehabilitation is to make a prosthesis, which is in harmony with the patient’s stomatognathic system.The inclination of the condylar path is the most important consideration in the oral rehabilitation. Condylar path is the path traversed by the condyle in relation to the articular eminence when the mandible is moved either protrusively or laterally from centric relation.[1] The condylar guidance is very important in edentulous patients. If not recorded accurately, it will lead to occlusal interference during mandibular movements.[2] The condylar guidance is basically defined as the mandibular guidance generated by the condyle and articular disk traversing the contour of the glenoid fossae.[3]
The condylar guidance in semiadjustable articulators is set either by individual protrusive or lateral interocclusal registrations[4],[5],[6]. The purpose of the protrusive jaw relation is to set the condylar elements of the articulator so they will reproduce inclinations, which are exact or nearer to the patients temporomandibular articulation[7]. The various methods used to record condylar guidance clinically are either extra-oral or intra- oral methods.Centric and eccentric relations can be recorded through intraoral or positional wax method, graphic recordings, functional recordings[8]. Gysi and McCollum generally gave the example of extra oral methods which mainly used in edentulous patients[9].
Several studies have shown the unreliability of recording and reproducing condylar guidance using these methods[10],[11]. Studies haveshown that average interocclusal registration values of the condylar guidance inclination vary from 21-64degrees[12]. Condylar guidance can also be recorded with radiographs, lateral cephalometrics, pantomograph, tomography, digital CT scans[13],[14],[15] and electronic axiography[16]. There are various articulator systems which vary in reproducing sagittal condylar guidance angulations. Studies for recording condylar inclination on various articulator systems in edentulous patients are very scarce. In this study two articulators have been used; one is Arcon( Hanau™ Wide-Vue 182-3 Articulator, Whip Mix Corporation, USA ) and another is Non-Arcon(Hanau™ H2 145 Articulator, Whip Mix Corporation, USA.) The purpose of this study to analyse the discrepancy between condylar guidance values obtained on these two articulators using protrusive records and the condylar guidance value on Orthopantomographs(OPG).
Materials And Methods
Patients
Before starting the study, ethical clearance was obtained from the institutional ethical board.
All subjects included in this study were screened through a detailed case history and were well informed regarding the study design. Written consent form from each of the subjects was obtained. A total of 20 completely edentulous subjects of either sex were selected for this study. Inclusion criteria for the subjects was patients in the age group of 40-55yrs, patients who had been completely edentulous only within the past 3 years, patients with good or fair condition of residual alveolar ridges and patients with class-1 jaw relation. Exclusion criteria was patients with Temporomandibular disorders, poor or resorbed ridges, poor general health and lack of adequate neuromuscular control of jaw movements
Clinical Methods
One set of upper and lower edentulous preliminary compound (Y-Dents® Impression Compound, MDM Corporation, Delhi, India)impressions were made for each subject and were poured in dental plaster (Kaldent, kalabhai Karson Pvt. Ltd, Mumbai India) following the manufacturer’s instructions and guidelines, giving a set of mandibular and maxillary cast for each individual. On the preliminary cast thus obtained, Autopolymerizing acrylic resin( DPI, Dental products of India; The Bombay Burmah Trading Corporation Ltd,India ) special trays were fabricated. Final zinc oxide eugenol(DPI,Dental products of India; Impression paste,The Bombay Burmah Trading Corporation Ltd,India ) impressions were made for each subject and were poured in Type-III dental stone (Gold Stone, kalabhai Karson Pvt. Ltd, Mumbai India) following the manufacturer’s instructions and guidelines. The master casts obtained were duplicated with agar material(Sindhu Ultramarine Chemicals pvt. Ltd,India). Heat cured Permanent denture bases(DPI, Dental products of India; The Bombay Burmah Trading Corporation Ltd,India) and wax record rims (Y-Dents®no.2, Modelling wax,MDM Corporation,Delhi,India) were fabricated on the original master casts as well as the duplicated master casts. Thus two sets of record blocks were obtained for recording maxillomandibular relations on each of the two articulators.
In this study two semiadjustable articulators were used Hanau Wide Vue and Hanau H2 Articulator [Figure 1a & b]. Facebow registrations for both the Semiadjustable articulators(H2 And Wide Vue) were accomplished using the standard technique as per the manufacturer’s instructions, with Axis Orbitale as a reference plane and orbitale as an anterior point of reference. Zeroing of both articulators was done(700 Sagittal and 0o Lateral condylar inclinations for H2; 30o Sagittal 30o Lateral condylar inclinations for Hanau Wide Vue). The facebow system used for H2 articulator was (The Hanau™ Earpiece Facebow ,Whip Mix Corporation, USA) and for Wide vue was(HanauTM Springbow, Whip Mix Corporation, USA ).
 | Figure 1(a) : Armamentarium for Hanau Wide Vue system
 |
 | Figure 1(b) : Armamentarium for Hanau H2 system
|
After the facebow transfer on both the articulators, maxillary casts were secured with plaster(Kaldent,kalabhai Karson Pvt. Ltd, Mumbai India)and mounted on the respective articulators. For each patient, for each articulator system, a centric jaw relation was recorded, and mandibular casts were mounted on the two articulators. A set of Hight extraoral tracers were attached to each set of record rims on both the articulators. The patient was trained to give a set of Gothic arch tracing on both sets of tracers. Intraoral centric and protrusive records (6mm from centric) were made with plaster(Kaldent,kalabhai Karson Pvt. Ltd, Mumbai, India) [Figure 2] for each patient for both the articulators.
 | Figure 2 :Centric and Protrusive Interocclusal records.
|
The lower cast was remounted on each articulator for each patient according to the new cenric relation record obtained from the tracing. The tracing plates were detached from the occlusal rims, keeping the central bearing plates with the intervening protrusive interocclusal record in place.
The two protrusive records were used to program each of the articulators respectively. Each of the protrusive interocclusal record was occluded between the respective recordings bases on each of the articulators, and then condylar locks of the articulators were rotated. For both articulators, the condylar balls on the articulator were raised or lowered, until the maxillary occlusal rim settled into stable position in protrusive relation. Condylar elements of the articulators were adjusted to get protrusive relation and with this we set horizontal condylar inclinations on both sides of both the articulators (Hanau Wide Vue and Hanau H2). The right and left sagittal condylar guidance values on both articulators were tabulated. The entire procedure was carried out by the same operator for all patients on both the articulators.
Radiographic Methods
An Orthopantomograph (OPG) of the jaws with the rims and protrusive interocclusal record insitu to hold the mandible in protruded position was made for each patient. The images of the OPG were printed . The sagittal outlines of the left and right articular eminence and glenoid fossae were traced on a transparent acetate tracing sheet by the examiner. The left and right "orbitale" (lowest point in the margin of the orbit) and " porion" (highest point in the margin of the auditory meatus) were identified and the Frankfort horizontal plane was constructed by joining the two landmarks on each side. The most superior point on the articular eminence and the most inferior point on the articular tubercle were identified and a second line to represent the mean condylar path inclination was constructed by joining the two points. The angle formed by the intersection of the two lines was determined to represent the angle of sagittal condylar inclination.[Figure 3][Figure 4]This was determined by the examiner and the average was taken as thetrue value.
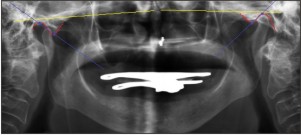 | Figure:3 : OPG(Orthopantomograph) tracing showing angle of the sagittal condylar guidance.
|
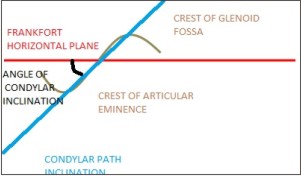 | Figure:4 : Line diagram of the OPG (Orhtopantomograph) tracing of the angle of sagittal condylar guidance
|
The data recordings comprised of three values for each of the 20 patients: the sagittal condylar inclinations obtained by programming the Hanau H2 and Hanau Wide Vue articulator, and the sagittal condylar inclination obtained from the OPG. The data thus obtained was tabulated and subjected to ANOVA test for group comparison. For multiple comparison Tukey HSD Test was done. The statistical analysis was done using SPSS(stastistical Package for the Social Sciences, IBM Software Group, USA) Version 17.0 software program.The results obtained were considered highly significant when P<0.01, significant when P<0.05, and were considered non-significant if the P value was more than 0.05.
Results
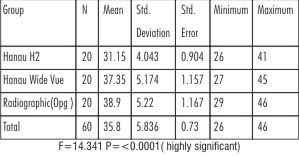
Table 1 and 2 show the mean and standard deviation of the sagittal condylar guidance values on right and left side respectively for 20 subjects(N),obtained by Hanau H2,Hanau Wide Vue, and Orthopanto mograph (OPG) tracings. The mean sagittal condylar guidance values for Hanau H2, Hanau Wide Vue and Orthopantomograph(OPG) tracings were 29.70±4.868 degrees, 35.45±4.696 degrees, 37.90±3.892 degrees on the right side and 31.15±4.043 degrees, 37.35±5.174 degrees, 38.90±5.220 degrees on the left side.[Figure 5]
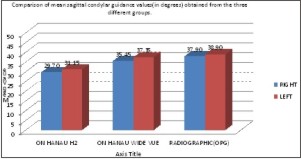 | Figure:5 : Comparison of mean sagittal condylar guidance values(in degrees) obtained from the three different groups.
|
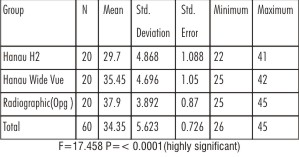 | Table 1: Mean sagittal condylar guidance values of the three different groups on the right side(in degrees)
|
 | Table 2: Mean sagittal condylar guidance values of the three different groups on the left side(in degrees)
|
Table 3 and 4 show the mean difference in sagittal condylar guidance values on the right side and left side respectively.The mean difference in sagittal condylar guidance value between Hanau H2 and Hanau Wide Vue articulators was found to be highly significant (P=<0.0001) on the right side and left side(P=<0.0001). The mean difference in sagittal condylar guidance values between Hanau H2 and Orthopantomograph tracing was found to be stastically highly significant with on right (P=<0.0001)and left side (P=<0.0001) respectively. A non significant difference in mean sagittal condylar guidance values was found between Hanau Wide Vue and Orthopantomograph on right side (P=0.207) and on left side respectively (P=0.572)
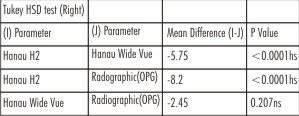 | Table 3: Intercomparison of mean sagittal condylar guidance values of the three different groups on right side(in degrees)
|
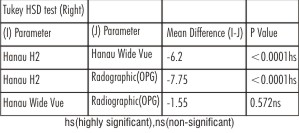 | Table 4: Intercomparison of mean sagittal condylar guidance values of the three different groups on the left side (in degrees)
|
Table 5 shows intra-group comparison of sagittal condylar guidance values obtained from three different groups. Mean sagittal condylar guidance values obtained from Hanau H2 and Hanau Wide Vue on the right and left sides were stastistically non significant with( P=0.312) and (P=0.231) respectively.
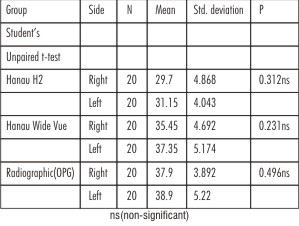 | Table 5: Intragroup comparison of sagittal condylar guidance values of the three different groups on the right and left sides(in degrees)
|
Discussion
During any Prosthodontic rehabilitation, it is very important to restore the patients’ occlusion so that it coincides with the centric relation.The condylar guidance is the angle at which the condyle moves away from a horizontal reference plane from centric relation along the articular eminence of mandibular fossa. The range of horizontal condylar guidance values were 30-35 for the Hanau H2( nonarcon) and 25-45 for the Hanau Wide Vue(arcon) articulator;these values are in accordance with Payne[17].
The Semiadjustable articulators used were Hanau H2(Non Arcon) and Hanau Wide Vue(Arcon) with their facebows.Orbitale was used as Anterior point of reference in both the articulators for orientation of maxillary cast which gives three –plane position of maxillary cast on both the semiadjustable articulators.[18] After the maxillary casts were mounted centric relation records were used to mount the mandibular cast. Hight extra-oral tracer were attached to the record rims. After gothic arch tracings, centric and protrusive records were made. Protrusive records were obtained at a 6mm distance from centric relation in the tracing. Acccording to one author horizontal condylar guidance changes with amount of protrusion, so it was important to keep the distance of protrusion same.[19] Posselt et al[20] also reported that correlation exists between degree of protrusion that can influence the setting of condylar readings. In the present study the amount of protrusion was same as the same protrusive records used for both the articulators.[21]
The panoramic radiographic image (orthopantomograph) was selected to obtain individual sagittal condylar guidance value which was considered as a standard for comparison with the two articulator groups. The panoramic radiographic image of the sagittal outline of the articular eminence and glenoid fossa was clearly identified in 20 subjects. When viewing the region of the temporal bone on OPG two radiopaque lines are apparent, the lighter and superior one depicting the the articular eminence and fossa; and the heavier, more inferior one representing the inferior border of zygomatic arch.
A difference in the sagittal condylar guidance values was noted between both the articulators. The mean sagittal condylar guidance values for the Hanau H2 (Non-Arcon) on the right side was 29.70±4.868 and on the left side was 31.15±4.043 degrees. The mean value for Hanau Wide Vue(Arcon) on the right side was 35.45±4.696 and on the left side was 37.35±5.174 degrees [Table 5]. These values are not statistically not significant but clinically condylar guidance values on the right side were slightly less than the left side in both the articulators.
These results are similar to those obtained in studies done by Arthur[22] and Gheriani and Winstanley[23]. This may be due to the anatomy of the condyle and glenoid fossa which dictate the condylar guidance, as it is determined by the distal slope of the Articulator eminence. Steeper the curvature of the condyle, greater will be the condylar guidance, and vice-versa. Inspite of a normal anatomy, the guidance may not be accordingly steep, as the condylar guidance is also affected by the ligament, muscle and soft tissues of the temporomandibular joints. The masticatory habits of the individual chewing pattern may also be responsible,as most subjects favour their right side for chewing which consequently leads to greater wear of the right condyle as compare to the left.
While comparison was made between the Hanau H2 articulator and Hanau Wide Vue Articulator in the present study, the mean difference for sagittal condylar values was 5.750 and 6.200 on right and left sides respectively, and this difference was highly significant for both right and left sides respectively. According to Shillinberg et al[24] and Rosenstiel et al[25] with the non-arcon design condylar inclination of the mechanical fossae changes in relation to the maxillary occlusion plane as the articulator is open and can lead to errors when a protrusive record of certain thickness is being used in program the articulator. They reported that with a 3 to 5 mm thickness of interocclusal record there would be a difference of 8o between where the articulator settings are adjusted and closed position where the articulator is used. Thus the average thickness of centric and protrusive interocclusal record must be within the range of 3-5 mm depending on the type of interocclusal record material, While comparing sagittal condylar guidance values obtained from Hanau Wide Vue and OPG readings, a mean difference of 2.45o and 1.55owas found on the right and left side respectively, which was statistically non significant [Table 3 and Table 4]. According to one study of the condylar movements, it was confirmed that in protrusion,the condylar head follows closely the anatomical form of the articular eminence and represents a very high correlation coefficient and level of significance[26]. According to Isberg at al [27], a high degree of correlation exits between the protrusive condylar path and the steepness of articular eminence, which may be attributed to the active role played by the soft tissues during condylar movements. Stallard and Stuart[28] propose that the muscles operating the mandible hold the condyles against the eminence throughout all condylar movements and these movements are guided by ligaments.Gilboa et al, reported a high degree of correlation between articular morphology and panoramic images and suggested that the inclination of the articular eminence in a panoramic image may be of value in setting the condylar guidance in semiadjustable articulators, which supports the present study.The correlation between mean sagittal readings of the Hanau Wide Vue articulator and radiographic(OPG) readings could be possibly due to the antomic representation of the articulator design in close approximation with the human temporomandibular joints.
Conclusion
From the results obtained from the study it may be concluded that the mean difference in sagittal condylar guidance values obtained from Hanau H2 and Hanau Wide Vue articulators
were highly significant indicating a low level of reproducibility. On the other hand the mean difference in sagittal condylar guidance values obtained from H2 articulator and OPG tracings was statistically highly significant whereas the mean difference in sagittal condylar guidance values obtained from wide vue and OPG tracings were non- significant. In the articulator groups studied, there was no significant difference in the condylar guidance values on the right and left sides, however slightly less value on the right side were observed.
References
1. Isaacson D. A clinical study of the condyle path. J Prosthet Dent 1959;9:927-35.
2. Pelletier LB, Campbell SD. Comparison of condylar control settings using three methods: a bench study. J Prosthet Dent. 1991;66:193–200.
3. The Glossary of Prosthodontic Terms. J Prosthet Dent2005;94:10-920
4. Posselt U.physiology of occlusion and ehabilitation. 2nd ed.Oxford:Blackwell Science,1968.p.121-32
5. Zarb GA Bolendar CL.Prosthodontictreatment for edentulous patients:complete denture and implant supported prostheses.12th ed. st.louis:Mosby;2004.p.294
6. Rosensteil SF,Land MF,Fujimoto J.Contemporary fixed prosthodontics.4th ed.St Louis:Mosby;2006.p.71.
7. Rothstein JR. Condylar guidance setting on articulators from protrusive records. J Prosthet Dent 1972;28:334-5.
8. Preti G, Scotti R, Bruscagin C, Carossa S. A clinical study of graphic registration of the condylar path inclination. J Prosthet Dent 1982;48:461-6.
9. Hickey JC, Zarb GA, Bolender CL. Boucher's prosthodontic treatment for edentulous patients. 9th ed. St. Louis: CV Mosby; 1985. p. 415.
10. Gross M, Nemcovsky C, Friedlander LD. Comparative study of condylar settings of three semiadjustable articulators. Int J Prosthodont. 1990;3:135–141.
11. Gross M, Nemcovsky C, Tabibian Y, Gazit E. The effect of three different recording materials on the reproducibility of condylar guidance registrations in three semi- adjustable articulators. J Oral Rehabil. 1998;25:204–208.
12. Gysi practical application of research results in denture construction.J Am Dent Assoc 1929;16:199-223.lundleen HC, Shyrock EF,Gibbs CH.An evaluation of mandibular border movements:their character and significance.J Prosthet Dent 1978;40:442-52
13. Dos Santos Júnior J, Nelson SJ, Nummikoski P. Geometric analysis of occlusal plane orientation using simulated ear-rod facebow transfer. J Prosthodont. 1996;5:172–181.
14. Christensen LV, Slabbert JC. The concept of the sagittal condylar guidance: biological fact or fallacy? J Oral Rehabil. 1978;5:1–7.
15. Gilboa I, Cardash HS, Kaffe I, Gross MD. Condylar guidance: correlation between articular morphology and panoramic radiographic images in dry human skulls. J Prosthet Dent. 2008;99:477–482.
16. Olivier Hue. Condylar path during protrusion in Edentulous Patients:Analysis with Electronic Axiography.
17. Payne JA, Condylar determinants in a patient population:Electronic pantographic assessment. j oral rehabil 1997;24:157-63.
18. Santos JD, Nelson SJ,Nummikoski P.Geometric analysis of occlusal plane orientation using simulated ear-rod face-bow transfer. j prosthodont 1996;5:172-81.
19. Craddock FW. The accuracy and practical value of records of condylar path inclinations. J Am Dent Assoc 1949;38:697-710.
20. Posselt U, Odont DR, Franzen G. Registration of the condyle path inclination by intraoral wax records:variations in three instruments. J Prosthrt Dent1960;10:441-53.
21. Weinberg LA. An evaluation of face- bow mounting. J Prosthet Dent 1960;10:620-30
22. Aull AE, condylar determinants of occlusal patterns. J Prosthet Dent 1965;15:826-46
23. Gheriani AS, W INSTANLEY rb.Graphic tracings of condylar paths and measurements of condylar angles. J Prosthet Dent 1989;61:77-87.
24. Shillinburg T, Herbert T, Hobo S, Whitsett LD, Jacobi R, Brackett SE.,et al. Fundamentals of fixed prosthodontics. 3rd ed. Illinois:Quintessence Publishing C; 1997. P. 42-81.
25. Rosensteil SF, Land MF, Fujimoto J. Contemporary fixed prosthodontics. 4th ed.. St. Louis: Mosby; 2006. P. 71-84.
26. Corbett NE, DeVincenzo JP, Huffer RA, Shryock EF.The relationship of the condylar path to the articular eminence in mandibular protrusion.J Prosthet Dent 1971;41:286-92.
27. Isberg A, Westesson PL. Steepness of articular eminence and movement of the condyle and disk in asymptomatic temporomandibular joints. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:152-57.
28. Stallard H, Stuart CE. Concepts of occlusion. Dent Clin North AM 1963;7:591-60.
|