Introduction
The three phases of root canal treatment comprise of chemo-mechanical preparation, disinfection and obturation of root canal space[1]. A primary objective of root canal therapy is complete obturation of the root canal space with the aim of sealing as much of the cleaned and shaped root canal system as possible[2],[3]. The difficulty in adequately obturating the root canal system is ascribed to its anatomical complexity and peculiar morphological configuration, which includes multiple foramina, apical deltas, accessory and lateral root canals. Since these components may constitute a pathway for passage of bacteria and products of tissue degradation between the root canal space and the surrounding periodontal system consists of an essential approach to yield the healing of periapical tissues[4].
Gutta-percha has been used in dentistry for over 150 years[4] and has become the most commonly used obturation material[5]. Traditionally, gutta-percha has been placed and compacted with a cold lateral technique[6]. In 1967, Schilder[3] described warm vertical compaction as an alternative to cold lateral condensation with the idea that compaction of thermoplasticized gutta-percha would permit full adaptation of the gutta-percha to the anatomic complexities of the root canal. Numerous modifications have been introduced for vertical compaction of gutta-percha[7]and backfilling with thermoplasticized, injectable gutta-percha[8]. More complete obturation of the main root canal and accessory canals and foramina may have a significant impact on the overall success rate of endodontic treatment[3].
Guttaflow was developed by Coltène Whaledent using modern expertise in silicone polymer technology. It is a cold, fluid obturation system that combines sealer and gutta-percha in a single material. It consists of a polydimethyl siloxane matrix which is highly filled with very finely ground gutta-percha and nano silver. The sealer part of Guttaflow is highly thixotropic, and with its fine grain size (<9 µm), the material flows well under slight pressure into the finest lateral canals.
The purpose of our study is to evaluate the movement of gutta-percha and Guttaflow into lateral grooves and depressions in the apical 7 mm of a split tooth model using gutta-percha as an apical plug.
Materials And Method
This study was conducted in the Department of Conservative Dentistry and Endodontics in S.G.T. Dental College. An extracted human maxillary canine with single, straight canal was used to create a split tooth model. The crown was removed and working length was established 1 mm from the anatomic apex. Pre-flaring of the coronal third was done using #3 and #4 gates glidden drills. The apex was prepared to a .04 taper size #40 at the working length.The tooth was then embedded in acrylic resin and four holes were placed in the acrylic model in the buccal lingual direction, two on the mesial and two on the distal surface. The tooth was then separated into buccal and lingual halves through the centre of the canal using a microtome. Lateral canals were placed on the buccal half of the model at 3, 5,7mm from working length using a diamond disc. Depressions were made at the same levels using a half round bur. The two halves were re-approximated using four bolts that fit tightly into the predrilled holes. A 2mm apical plug with 0.04 % gutta-percha was created. The model was kept at 37S04;C at all times between obturations. Three experimental groups were included as follows:
Group I = GuttaFlow (GF)
Group II = System B plugger inserted to 5 mm from working length (Gp5)
Group III = System B plugger inserted to 3mm from working length (Gp3).
The model was irrigated with 15% EDTA and 5.25% NaOCl followed by final rinse with isopropyl alcohol. The canal was dried with paper points. Ten obturations were performed for each group.
Guttaflow plastic tip was inserted into the canal to a depth at which the tip no longer advanced. GuttaFlow capsule was activated for 30 seconds and the material was dispensed until it could be seen moving out of the canal around the tip. All obturations with gutta-percha were performed using system B continuous wave condensation with gutta-percha cones and sealer. Backfilling was performed with Obtura II set at 200S04;C. After each obturation the model was separated into its facial and lingual halves. The halves were viewed and photographed at X10 magnification. (Fig. 1)
 | Fig 1. : Gutta Flow
 |
Evaluation of obturation of lateral grooves and depressions at 3mm and 5mm was scored as follows:
0= no gutta-percha or Guttaflow in grooves and depressions.
1= presence of gutta-percha or Guttaflow in grooves and depressions.
Statistics
Statistical analysis was performed by using Friedman’s test to evaluate for differences between 3 treatment groups. Where appropriate, Wilcoxon signed rank test was used to make comparisons between two treatment groups and within each group.
Results
Results of the study showed that Guttaflow flowed into all depressions and lateral grooves in the apical 5 mm of the split-tooth model. In the apical 3 mm of the model, the material was significantly better than gutta-percha in obturating lateral grooves and depressions regardless of the depth of insertion of the System B plugger. Better flow of material was seen at the 3-mm level for Guttaflow than gutta-percha when the System B plugger penetrated to 5 mm from the working length. (Table 1 and 2) Guttaflow resulted in no extrusion of material beyond the apex in 100% of obturations. However according to the study conducted by TM Zielinski et al[1] Guttaflow resulted in extrusion of material as no apical barrier was used. Intergroup comparison at different groove levels showed that GuttaFlow had significantly better flow than guttapercha into grooves at 3mm level when the when the plugger was inserted to 5mm from the WL.
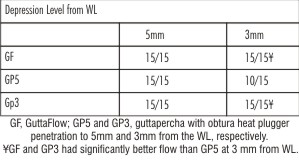 | TABLE 1 : Number of Specimens with Flow of GuttaFlow or Gutta-Percha into Each Depression at the Various Levels from the WL
|
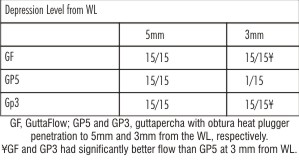 | TABLE 2 : Number of Specimens with Flow of GuttaFlow or Gutta-Percha into Each Depression at the Various Levels from the WL
|
Discussion
The purpose of this ex vivo study was to compare the flow of GuttaFlow and gutta-percha into depressions and lateral grooves in the apical half of a split-tooth model. The use of the same split-tooth model for all obturations and monitoring of material placement and compaction forces ensured standardization of each obturation among the four experimental groups. Clinical conditions of temperature and humidity were maintained throughout the experiment.
GuttaFlow flowed into all depressions and lateral grooves in the apical 5 mm of the split-tooth mode, coronal to the apical plug. Better flow of material was seen at the 3-mm level for GuttaFlow than gutta-percha when the System B plugger penetrated to 5 mm from the WL.
The tendency for GuttaFlow to extrude beyond the apex raises concerns regarding cytotoxicity. All sealers are initially cytotoxic[9],[10],[11],[12], with little cytotoxicity noted after 24 hours[13]. A study performed by Bouillaguet et al.[14] found that set GuttaFlow was significantly less cytotoxic than set AH Plus (Dentsply/Maillefer, Konstanz, Germany), Epiphany sealer (Pentron Clinical Technologies, LLC, Wallingford, CT), and Resilon (Pentron Clinical Technologies) at 24 hours and 48 hours. Hence, an apical plug of 2mm was created with guttapercha.
Studies evaluating the sealability of GuttaFlow have shown conflicting results. Using a bacterial leakage model, Monticelli et al.[15]showed that teeth obturated with GuttaFlow had an inferior seal against bacterial leakage compared with teeth obturated with gutta-percha and AH Plus by using a warm vertical technique. In contrast, Brackett et al.[16]found no significant difference in sealing ability between GuttaFlow and vertically compacted, thermoplasticized gutta-percha and AH Plus sealer when using a fluid filtration technique. The variability in results may be attributed to differences in the methods of leakage assessment.
The manufacturer claims that GuttaFlow achieves a final set within 25 minutes to 30 minutes after trituration of the GuttaFlow capsule regardless of temperature or humidity[17]. Based on data obtained during a pilot study, it was found that the material did not set in either the split-tooth model or on the bench top after 30 minutes or 40 minutes and inconsistently set after 45 minutes. Because the material was only found to set consistently after 50 minutes, the split-tooth model was kept in the incubator for 50 minutes after each obturation to ensure complete set of the GuttaFlow.
The split-tooth model was irrigated with isopropyl alcohol before obturation with GuttaFlow as the manufacturer suggests because of the fact that residual chemicals within the canal system may impede setting of the material[17]. In a pilot study, GuttaFlow failed to set after more than 1 hour in the incubator in cases in which the model was irrigated with NaOCl as the final rinse.
The insufficient softening of the gutta-perchaby heat could be responsible for low gutta-percha adaptation and flow in the lateral grooves as compared to Gutta Flow. A low percentage of gutta-percha polymer could result in reduced plasticity and a decreased flow rate of the filling material.
It is important to highlight that this study utilized teeth with straight roots and single canals, whereas most posterior teeth have a more complex anatomic configuration with a number of isthmus, curvatures and foramina. Even so, we expect that the findings of this study may widen the scopes, on the filling of lateral canals and prompt the development of further researches.[4] Subsequent studies could further develop the existing model to include depressions and grooves of varying sizes as well as different master apical file sizes and tapers and varying canal curvatures.[5]
According to various studies conducted maximum number of lateral canals are in the apical third of the roots. In this study we made an apical plug of 2mm with gutta-percha. This may have resulted in non sealing of lateral canals in apical 2 mm of the root.
Conclusion
Within the limitations of this in-vitro study it can be concluded that Guttaflow flows significantly better in the apical 3 mm of a split-tooth model than gutta-percha placed using a warm vertical technique.
References
1. Zielinski T M, Baumgartner J C, Marshall J G. Guttaflow and Gutta-Percha for Filling Lateral Grooves and Depressions.J Endod 2008;34(3):295-298.
2. H. Schilder. Vertical compaction of warm gutta-percha H. Gerstein (Ed.), Techniques in Clinical Endodontics, Saunders, Philadelphia (1983), pp. 76–98
3. H. Schilder. Filling root canals in three dimensions Dent Clin North Am, 11 (1967), pp. 723–744
4. Barroso J M, Carrasco L D, Capelli A,Guerisol D M Z, Saquy P C, Pécora J D. Influence of gutta-percha points on thefilling of simulated lateral canals.J Applied Oral Sci 2005;13(2):176-179.
5. A. Goodman, H. Schilder, W. Aldrich. The thermomechanical properties of gutta-percha IIThe history and molecular chemistry of gutta-percha Oral Surg, 37 (1974), pp. 954–961.
6. J. Taintor, P. Ross. Opinions and practices of American endodontic diplomats. Can Dent J, 44 (1978), pp. 321–325.
7. L.S. Buchanan. The continuous wave of condensation technique: a convergence of conceptual and procedural advances in obturation.Dent Today, 13 (1994), pp. 80–85
8. F.S. Yee, J. Marlin, A.A. Krakow, P. Gron. Three-dimensional obturation of the root canal using injection-molded, thermoplasticized dental gutta-percha.J Endod, 3 (1977), pp. 168–174
9. B.M. Briseno, B. Willershausen Root canal sealer cytotoxicity on human gingival fibroblastsI. Zinc oxide-eugenol-based sealersJ Endod, 16 (1990), pp. 383–386.
10. B.M. Briseno, B. Willershausen Root canal sealer cytotoxicity on human gingival fibroblastsII. Silicone- and resin-based sealers.J Endod, 17 (1991), pp. 537–540.
11. B.M. Briseno, B. Willershausen Root canal sealer cytotoxicity with human gingival fibroblastsIII. Calcium hydroxide-based sealers. J Endod, 18 (1992), pp. 110–113.
12. L. Spangberg, K. Langeland. Biologic effects of dental materials. 1Toxicity of root canal filling materials on HeLa cells in vitro. Oral Surg, 35 (1973), pp. 402–414.
13. K.E. Safavi, L.S.W. Spangberg, N.S. Costa, G. Sapounas. An in vitro method for longitudinal evaluation of toxicity of endodontic sealers.J Endod, 15 (1989), pp. 484–486.
14. S. Bouillaguet, J.C. Wataha, F.R. Tay, M.G. Brackett, P.E. Lockwood. Initial in vitro biological response to contemporary endodontic sealers. J Endod, 32 (2006), pp. 989–992.
15. F. Monticelli, F.T. Sadek, G.S. Schuster et al. Efficacy of two contemporary single-cone filling techniques in preventing bacterial leakage. J Endod, 33 (2007), pp. 310–313.
16. M.G. Brackett, R. Martin, J. Sword et al. Comparison of seal after obturation techniques using a polydimethylsiloxane-based root canal sealer. J Endod, 32 (2006), pp. 1188–1190.
17. GuttaFlow instructions for useColtène/Whaledent Inc, Cuyahoga Falls, OH (2006) February
18. A. D. Kececi, G CelikUnal, B H Sen. Comparison of cold lateral compaction and continuous wave of obturation techniques following manual or rotary instrumentation. IntEndod J 2005;38(6):381-388
|