Introduction:
The fracture of heat cure denture bases is a common clinical occurrence. Autopolymerizing acrylic resin is commonly used for repair, as it facilitates a simple and quick repair. Chemical modifications of the fractured surfaces are done by applying chemical agents to ensure better bonding. Methacrylates (MMA), Organic solvents such as Chloroform, Acetone, and Methylene chloride arefew of the chemical agentsused for this process[1]. The purpose of this study is to evaluate the effect on transverse strength and modulus of elasticity of repaired denture base resin after chemical surface treatment.
Materials and Methods:
A standardized aluminum die measuring 65 × 10 × 3mmwas prepared according to ADA specification no.12 (Fig-1), for measurement of transverse strength and Flex modulus of a denture base resin.[2]
 | Figure 1 - Aluminium Die according ADA Sp.no.12
 |
The die was flasked in dental stone to obtain mould spaces which were used as matrices for the fabrication of heat polymerized acrylic resin specimens. Heat cure acrylic resin was packed into the mould spaces and acrylization was done. The resin specimens were finished to a size of 2.5 × 10 × 64 mm with 600-grit silicon carbide paper under water irrigation (Fig -2). All thespecimens were stored in water at 37ºC for 7 days before the surface treatments.
 | Figure 2 - Acrylic Specimens
|
The acrylic resin specimens were divided into 5 subgroups, each with 10 specimens. Group 1 -includes in methylene chloride (mc) for 30 seconds, Group 2 - in acetone (ac) for 30 seconds, Group 3-without any fracture (intact specimens) Group 4- had no surface treatment, Group 5 in MMA (mo) for 180 seconds. The prepared intact specimen was cut into half with a high speed diamond disk cutter under copious irrigation. Each surface was given a 45-degree bevel and polished with 600-grit silicon carbide with water irrigation. Specimens surfaces were treated with chemical etchants, by immersion in acetone,in methylene chloride or in MMA (Fig-3).
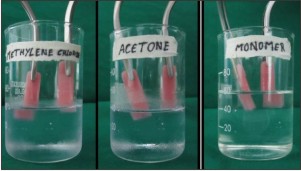 | Figure 3 - Chemical Surface Treatment of the specimens
|
After treatment of the cut surface, the heat-polymerizing strips were fixed in a stone mold to obtain a space for placing the repairing resin. Widths between half strips were 2 mm at the top and 6 mm at the bottom. The autopolymerizing acrylic slurry, which consisted of 10 g powder with 7.5 ml liquid, was infused into the space with the use of a vibrator to obtain specimens. The flasks were closed and placed under hydraulic pressure.
After the specimens were retrieved from the mold it is trimmed of the excess material .
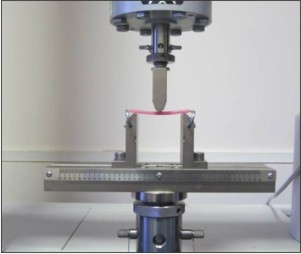
All specimens were stored in 37°C distilled water for 7 days before the test. Each specimen was subjected to the 3-point bending test at a crosshead speed of 5 mm/min at a 50-mm distance with an Instron test apparatus .The load was applied to the center of the 2-mm repaired area for the experimental groups and to the center of the control specimens at a 5.0 mm/min crosshead speed (Fig-4). Transvere strength, fracture load, modulus of elasticity and deflection values were automatically calculated by the software and the results were recorded.
 | Figure 4 - Testing the Specimen using Instron testing machine
|
The breaking load was converted to transverse repair strength (S) by the formula S = 3 PL/2 bd2, where P is the load at fracture, L is the length between the jig tips (50 mm), b is the width, and d is the thickness of the specimen.
Results:
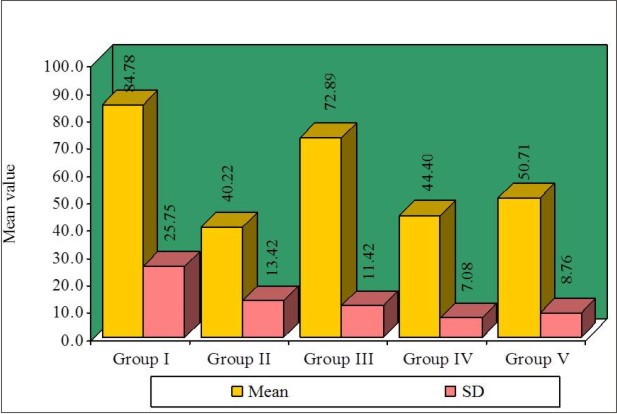
One-way ANOVA statistical analysis was used to determine whether significant differences existed between the means of the experimental groups (I, II, III, IV, V) with respect to Flex Modulus (Table-1) and Transverse strength (Table-2). Newman-Keuls multiple post hoc test was done for pair wise comparison of five groups (I, II, III, IV, V) with respect to Flex Modulus (Table-3) and Transverse strength (Table-4).
 | Figure 5 - Graphical representation of Newman-Keuls multiple post hoc for Flex modulus
|
 | Figure 6 - Graphical representation of Newman-Keuls multiple post hoc for Transverse Strength
|
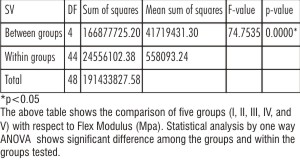 | Table 1
|
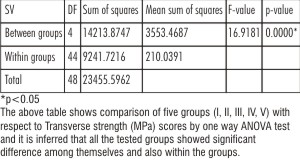 | Table 2
|
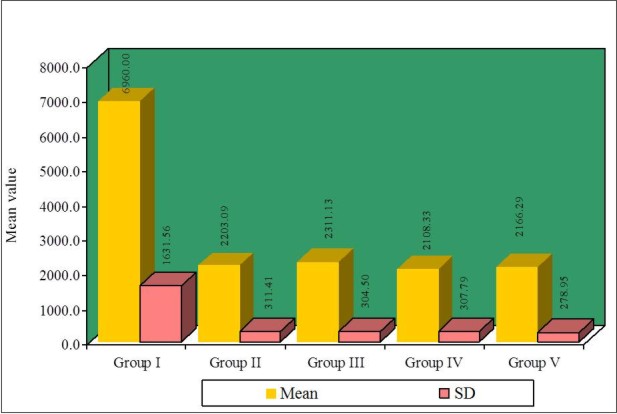
Among the 5 groups tested Group 1 (Specimens treated with Methylene chloride) showed highest flex modulus followed by Group 3 (Intact specimens), Group 2 (Specimens treated with Acetone ), Group 5 (Specimens treated with Methyl methacrylate) and finally Group 4 (Specimens without surface treatment) when statistically analyzed by one way ANOVA test and Newman-Keuls multiple post hoc procedure (Fig-5)
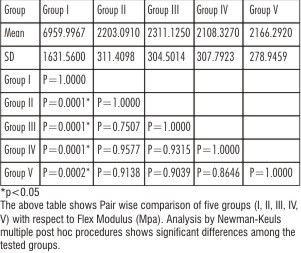 | Table 3
|
Among the 5 groups tested Group 1 (Specimens treated with methylene chloride)showed highest tranverse strength followed by Group 3(Intact specimens), Group 5 (Specimens treated with Methyl methacrylate), Group 4 (With out surface treatment) and finally Group 2 (Specimens treated with Acetone) when statistically analyzed by one way ANOVA test and Newman-Keuls multiple post hoc procedure (Fig-6)
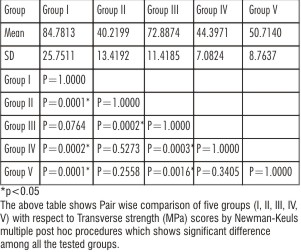 | Table 4
|
Discussion
Acrylic resin polymers were introduced as denture base material in 1937 and by 1946, 98 of all denture bases were fabricated with polymethyl methacrylate (PMMA)[3]. Today, inspite of advent of newer denture base materials in the market majority of denture bases are made with heat-cured PMMA polymers.
Despite of its popularity, the material is not without limitations. This is reflected in the unresolved problem of denture fractures and the accompanying costs of their repairs [4].
The fracture of poly (methyl) methacrylate denture bases is a common clinical occurrence. Denture fracture can occur outside or inside the mouth. The reasons for the fractures occurring outside the mouth could be due to accidents or falls as a result of expelling the denture from the mouth while coughing, or dropping the denture while handling and cleaning them. Causes of denture fractures occurring inside the mouth are related to inadequate fit of the denture base, poorly balanced occlusion, faulty design and fabrication, insufficient strength of the material, excessive bite force, improper occlusal plane, high frenal attachments, stress induced in the denture base following years in clinical use, and primarily in the midline of maxillary complete dentures when opposed by mandibular natural dentition[5], [6].
The clinician must often decide whether to repair or replace the broken denture. To minimize inconvenience to the patient and save cost in the reconstruction of the dentures, quick and reliable denture repairs are often opted.
However the repaired denture strength relies on the type of repair material used. Numerous materials like autopoly merising resin, heat cure resin, visible light cure, microwave cure have been used to repair dentures. Among which Heatcure & Autopolymerizing resins are commonly used. Clinically autopoly merising acrylic resin is the most commonly used material for repair because it is easy, quick, and inexpensive method having adequate strength, good color match.
Adhesion between denture base and repair material can be improved by applying appropriate chemicals to the acrylic resin surfaces .
Methyl methcrylate, Chloroform, Acetone, and Methylene chloride have been used as softening agents in several situations, including repair of denture bases because of its ability to dissolve the denture material, allowing improved bonding by forming an interpenetrating polymer network at the interface.
The purpose of this study is to evaluate the effect on Transverse strength and Modulus of elasticity of DPI Heatcure denture base resins repaired with commonly used DPI autopolymerizing resin after different chemical surface treatments.
The various chemical surface treatments used in this study were Acetone, Methylene chloride, and Heat cure monomer before the repairing procedure.
Shenin 1984 stated that wetting the denture base resin surface with chloroform for 5 seconds creates a cleaner and more efficient site for bonding, increasing the strength of denture repairs; however, chloroform was identified as a noxious compound with a carcinogenic potential, and precautions are necessary to avoid inhaling chloroform vapor during surface treatment. As a result, chloroform has been replaced by methylene chloride. It has been suggested that the wetting of methylene chloride on the surface causes crazing as well as the formation of numerous pits up to 2 μm in diameter.[7] In the present study also chloroform was not used to treat the specimens because of its carcinogenic property instead Methylene chloride was used.
Vallittu P K in 1994 investigated the transverse strength of the repaired test specimens of heat-cured acrylic resin after treating the specimens with methyl methacrylate for various amounts of time before the autopolymerizing acrylic resin was applied to the joint space. A three point loading test was used to determine the transverse strength of the test specimens. The results revealed that repaired test specimens were weaker than those unrepaired . The strength of the test specimens increased as the duration of methylmethacrylate wetting of the repair surface increased.[8] Nagai E in 2001 have studied Transverse strength and modulus of elasticity of repaired acrylic denture base specimens and evaluated with a 3-point bending test in comparision to a heat-polymerized control group. Autopolymerizing acrylic resin was used with and without methylene chloride surface treatment. Specimens without methylene chloride surface treatment showed lowest strength value 53.2 MPa & lowest elastic modulus 2567.3 MPa.[9]
Bural C in 2010investigated flexural properties of heat-polymerised acrylic resin specimens repaired with two types of resins after the repair surfaces were wetted with heat, autopolymerizing monomers and acetone for 180 s. After repairs, specimens were subjected to three-point bending test and flexural strength, strain, fracture load, modulus of elasticity and deflection values were recorded. Within the wetting agents, heat cure monomer and auto polymerising monomer producedthe best mechanical properties, while wetting with acetone did not provide superior effect over both monomers, they have concluded that in clinical use, wetting the repair surfaces may result in stronger repairs.[10] Thus chemical surface treatment of the repairing surfaces of denture base material have been proved to increase the bond strength thereby improving modulus of elasticity and transverse strength.
Conclusion:
Within the limitations of the study the following conclusions can be drawn.
Modulus of Elasticity:
1. Modulus of elasticity of the specimens treated with methylene chloride showed significant values when compared to all others groups,
2. The remaining groups, acetone and monomer did not show much significant difference among themselves.
Transverse Strength:
1. The transverse strength of methylene chloride treated specimens showed highest values among all the tested groups.
2. The transverse strength of monomer group when compared to the control group showed significant improvement. No much difference was shown by the acetone group when compared to the control group.
Methylene chloride pretreatment of the specimens can be effectively used during repair process of the denture bases to improve the transverse strength as well as modulus of elasticity of the repaired denture bases.
References
1. Minami H, Suzuki S, Minesaki Y, Kurashige H, Tanaka T.In vitro evaluation of the influence of repairing condition of denture baseresin on the bonding of autopolymerizing resins. J Prosthet Dent 2004;91:164-70.
2. Hanna EA,Shah FK,Gebreel AA.Effect of joint surface contours on the transverse and impact strength of denture base resin repaired by various methods. An In Vitrostudy. Journal of American Science 2010;6:115-25.
3. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy between compression and injection molded complete dentures. J Prosthet Dent 1999;82:291-300.
4. Stipho HD ,Stipho AS. Effectiveness and durability of repaired acrylic resin joints. J Prosthet Dent 1987;58:249-53.
5. Stipho HD. Repair of acrylic resin denture base reinforced with glass fiber. J Prosthet Dent 1998;80:546-50.
6. Seo RS, Neppelenbroek KH, Filho JNA.Factors Affecting the Strength of Denture Repairs. J Prosthodont 2007;16:302-10.
7. Shen C, Colaizzi F A, Birns B. Strength of denture repairs as influenced by surface treatment. J Prosthet Dent 1984;52:844-48.
8. Vallittu P K, Lassila V P, Lappalainen R. Wetting the surface with methyl methacrylate affects the tranverse strength of repaired heat-polymerized resin.J Prosthet Dent 1994;72:639-43.
9. Nagai E, Otani K, Satoh Y, Suzuki S. Repair of denture base resin using woven metal and glass fiber: Effect of methylene chloride pretreatment. J Prosthet Dent 2001;85:496-500.
10. Bural C et al. Flexural properties of repaired heatpolymerising acrylic resin after wetting with monomer and acetone.Gerodontology 2010;27:217-23.
|