Introduction:
Perforations can be defined as mechanical or pathologic communications between, the root canal system and the external tooth surface [1]. Root perforation is a communication between the root canal system and periodontal ligament through the floor of the pulp chamber or root canal wall. It can occur as a result of carious lesion, internal or external root resorptionduring endodontic instrumentation and post space preparation. The prognosis of an endodontic perforation depends on the size and location of the defect, and it will improve when it is sealedimmediately with abiocompatible and sealable material [1],[2],[3],[4]
Several materials have been used to repair furcation perforations, including zinc oxide-eugenol cements (IRM and Super-EBA), glass ionomer cement, composite resins, resin-glass ionomer hybrids, and mineral trioxide aggregate (MTA). MTA was developed at Loma Linda University in the 1990s as a root-end–filling material. Lee et al. [5] compared the sealing ability of MTA with that of amalgam and IRM in experimentally induced lateral perforations. They found that MTA had significantly less leakage. Torabinejad et al.[6] compared the sealing ability of MTA with that of amalgam and Super-EBA when used as root-end fillings. They showed that most of the MTA samples had no dye penetration.
The effect of time and moisture on setting, retention, and adaptabilityare the properties of a material will play important role in repair furcation perforations. The authors noted that the presence of moisture in perforations during the placement of MTA increased its adaptation to perforation wall and concluded that a moistened matrix can be used under MTA to prevent over- or underfilling of the material[7].MTA showed promise in this respect and could enhance the treatment modality for furcation perforation repair. Studies comparing MTA with Portland cement showed their similarity in composition, properties, and tissue reactions [8],[9].
Until recently, two commercial forms of MTA have be available; ProRoot MTA (Maillfer, Dentsply, Switzerland) is available in either the gray or white form. In our study we used white form of pro root MTA(in the article pro root MTA refers to white form of pro root MTA). According to the information supplied in the material safety datasheet, ProRoot MTA consists of 75% Portland cement, 20% bismuth oxide, and 5% calcium sulfate dehydrate. Recently, MTA- Angelus (Angelus, Londrina, PR, Brazil) has also become available as an alternative to ProRoot MTA. MTA-Angelus contains 80% Portland cement and 20% bismuth oxide, with no addition of calcium sulfate in an attempt to reduce setting timen (2 hours for ProRoot MTA and 10 minutes for MTA Angelus[10]. This has generatedscientific interest in the evaluation of Portland cement as a low-cost alternative to MTA, with recent studies comparing MTA with Portland cement. Both materials have beendemonstrating comparable physical and biologic properties as well as clinical outcomes.However, there are disadvantages when using both MTA and Portland cement, such asthe extended setting time and the difficulty of handling [11][12][13][14].
Several methods have been used to evaluate leakage of perforation repair materials including dye penetration [15], bacterial and fluid filtration [16] etc. A new method for leakage evaluation called the dye-extraction method when compared it with the classic dye penetration and fluid-filtration techniques, a statistically significant correlation was found between the resultsobtained with the dye extraction and those obtained with the fluidfiltrationtechnique [17].
The aim of this study was to evaluate the sealing ability of ProRoot MTA , MTA-Angelus,Portland cement and IRM when used to repair furcation perforations, with and without the use of internal matrix.
Materials And Methods:
One hundred human permanent lower first molars were used in this study. Collected teeth had minimal caries or restoration, and none had fused roots. Any tooth that had a crack or defect was discarded. Molars were amputated 3 mm below the furcation area by using a tapered diamond stone. Endodontic access cavity was made in every molar by using a high-speed long shank round bur #2 (#2RC; SybronEndo Europe, The Netherlands) for the initial entry followed by Endo-Z (Maillfer, Dentsply, Switzerland) for lateral extension and finishing of cavity walls. A temporary filling material (Cavit, 3M ESPE) was placed over the orifice of each canal. Every molar was covered completely including cavity walls and pulpal floor with two successive layers of clear nail varnish. A perforation was made between the orifices to the furcation area by using a high-speed round bur #2. Care was taken to centralize the perforation between the mesial and distal orifices (Fig. 1)
 | Figure (1): Tooth after creating the perforation
 |
Molars were divided into four experimenta (Group I- IV) land positive (Group-V) and negative (Group-VI)
Group:
(1) Group 1,20 molars in which perforations were repaired with ProRoot MTA;
(2) Group 2,20 molars in which perforations were repairedwith MTA-Angelus;
(3) Group 3,20 molars in which perforations were repaired with Portland cement ;
(4) Group 4,20 molars in which perforations were repaired with IRM
(5) Group 5,10 molars in which perforations were left unsealed (positive control); and
(6) Group 6,10 molars without perforation(negative control).
The four experimental groups were further subdivided into the following subgroups: subgroup a, 10 molars in which no internal matrix was used, and subgroup b, 10 molars in which internal matrix (collagen) was used. Molars were placed in Eppendorf tubes containing cotton moistened with saline in an attempt to stimulate clinical conditions. The molars were sealed to the tubes by using cyanoacrylate adhesive. The tubes were fixed in a table vise (PanaVise Products Inc, Reno, NV), and rubber dam (OptraDam, Vivadent, Germany) was placed. The repair procedure was performed under 14 Xusing surgical microscope (Opmi-Pico; Karl Zeiss, Jena, Germany).
In subgroups b, Internal matrix (ETIK; Pierre Rolland, Acteon,France) was adapted to interradicular area by using hand pluggers (Buchanan pluggers; SybronEndo Europe, Amersfoort, The Netherlands) [18]. ProRoot MTA, MTA-Angelus, portland cement and IRM were mixed according to the manufacturer instructions. They were applied to the perforation site in increments by using the microapical placement system (MAP, Produits Dentaires SA, Vevey, Switzerland) and lightly condensed using Buchanan pluggers . Moist cotton pellets were placed over the repair materials, and molars were kept in 100% humidity for 24 hours to allow materials to set. Molars were then placed in Petri dishes according to each group. Methylene blue dye was applied inside the access cavity of all samples for 24 hours. Molars were placed under running tap water for 30 minutes to remove all residues of methylene blue and then varnish was removed with a Parker blade #15 and polishing discs.
Molars were placed in vials containing 1mL of concentrated (65 wt%)nitric acid for 3 days (Fig. 2). Vials were centrifuged (Universal 16R; Hettich Zentrifugen, Tuttlingen, Germany) at 14,000 rpm for 5 minutes. Two hundred microliters of the supernatant from each sample was transferred to a 96- well plate. Sample absorbance was read by an automatic microplate spectrophotometer (E 960, Bioblock, Starsbourg, F) at 550 nm using concentratednitric acid as the blank.
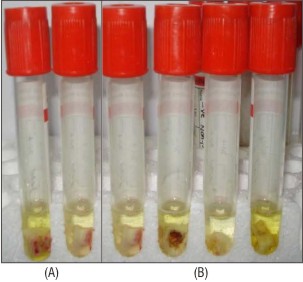 | Fig(2). : Molar placed in vials containing 1mL of concentrated (65 %) nitric acid, (A) +ve control & -ve control group, (B) Experimental groups
|
Statistical Analysis:
Statistical analysis was performed by using one-way analysis of variance. A Duncan post hoc test was used for pair-wise comparison between the means when analysis of variance test was significant. The significance level was set at p < 0.05. Statistical analysis was performed with SPSS 16.0 (Statistical Package for Scientific Studies, SPSS, Inc., Chicago,IL, USA) for Windows.
Results:
The positive control showed the highest dye absorbance (0.7+ 0.1). IRM without internal matrix (0.23 + 0.05) came second withsignificantly higher dye absorbance than other groups Portland cement with (0.125+ 0.06) and with out matrix(0.168 + 0.09.) and MTA-Angelus with(0122 + 0.06)and without matrix (0.167 +0 07) had no significant difference in between them;and IRM with internal matrix (0.0.169 + 0.07). was showed significantly higher absorbance than the other remaining groups. ProRoot MTA with(0.112 + 0.09.) and without matrix (0.115 + 0.07) showed less dye absorbance and there is no significant difference between them. However, they were significantly higher than the negative control group (0.066+ 0.01) (p>0.05) (Table.1).
 | Table 1. A histogram showing the mean dye absorbance values of different groups.
|
Discussion
The dye-penetration technique has long been used in endodontics because of its ease of performance and difficulty of other available techniques. However, it has several drawbacks including the smaller molecular size of the dye molecules than bacteria, which do not measure the actual volume absorbed by the sample but merely measure the deepest point reached by the dye [17]. It relies on randomly cutting the roots into two pieces, without any clue of the position of the deepest dye penetration [17]. Despite these drawbacks, Torabinejad et al.[6] stated that a material that is able to prevent the penetration of small molecules (dye) should be able to prevent larger substances like bacteria and their byeproducts. Based on this, the dye-extraction method seems to be a reliable technique. It takes into account all absorbed dye by the samples. Camps and Pashley[17] reported that the dye-extraction method gave the same results as the fluid-filtration method and also saved much laboratorytime.
Furcation perforations were induced by a #2 long shank carbide round bur from pulpal floor to furcation area. This resulted in perforations of almost 1 mm in diameter [19] Internal matrix has been advocated by Lemon [18] to limit the overextension of the repair material. The collagen matrix used in this study is a soft material, which expands because of moisture and has a hemostatic effect. It seems suitable to be used with MTA and IRM because these materials are pastes and do not require forces of condensation as stated by Bargholz[20]. Negative control samples had low dye absorbance (0.066) close to that of blank (nitric acid), which showed absorbance of 0.043. This small difference can be attributed to the yellowish color of teeth, whereas blank is colorless. Positive control samples in which perforations were not repaired had the highest dye absorbance of all groups denoting the accuracy of the technique [19]. Pro Root MTA has been proven to have less leakage and has produced a better response compared to other materials and our study got similar results as with Lee et al [21].
MTA Angelus and Portland cement have comparable sealing ability[22]. ProRoot MTA with and without matrix showed almost the samedye-absorbance results, so that the use of matrix with ProRoot MTA seems not necessary as previously mentioned by Arens and Torabinejad [23]. Being hydrophilic and easily adapted to cavity walls may be the main reasons for this similarity in dye absorbance between the two subgroups. Contrary to ProRoot MTA, MTA-Angelus showed significantly higher dye absorbance when used without matrix. This could be explained by the difference in composition between ProRoot MTA and MTA-Angelus. MTA-Angelus does not contain calcium sulfate and has lower percentage of bismuth oxide as stated by Song et al.[24]. This resulted, according to the manufacturer, in a reduction of the setting time from 2 hours for ProRoot MTA to 10 minutes for MTA-Angelus[7]. However, this reduction in the setting time may have prevented MTA-Angelus from having better wetting and adaptation to cavity walls this needs further investigation.
Portland cement with and without matrix had no significant difference in dye absorbance as compared with MTA Angelus. In agreement with the results of the present study, previous reports have demonstrated that MTA Angelus and Portland cement have comparable sealing ability[25],[26]. IRM with & without matrix showed the highest dye absorbance of all experimental groups. The presence of matrix significantly decreased the dye absorbance of IRM. So that the internal matrix willprevent overextension and control moisture, which will lead to moreadaptation, resulting in better sealability.
Conclusion
With in the limitations of our present invitro study, the following conclusions can be drawn:
(1) Neither cement was capable of producing a fluid-tight seal;
(2) The use of IRM to repair furcation perforations should be limited, and, if used, it must be used with an internal matrix.
(3) ProRoot MTA has excellent sealing ability and can be used with or without matrix in repair of furcation perforations.
(4) MTA Angelus and Portland cement has near comparable results in preventing microleakge .
(5) The present results suggest that Portland cement has the potential to be developed as a furcal repair material, but more studies are necessary before warranting unlimited clinical use.
References:
1. Seltzer S, Sinai IH, August D. Periodontal effects of root perforations before and during endodontic procedures.J Dent Res 1970;49:332-336.
2. Daoudi M. Microscopic management of endodontic procedural errors: Perforation repair. Dent Update 2001;28:176-180.
3. American Association of Endodontists glossary of endodontic terms, 7th ed. Chicago,IL: American Association of Endodontics, 2003.
4. Bryan EB, Woollard G, Mitchell WC. Nonsurgical repair of furcal perforations: A literature review. Gen Dent 1999;47:274–8.
5. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod 1993;19:541– 4.
6. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as root end filling material. J Endod 1993;19:591–5.
7. Sluyk SR, Moon PC, Hartwell GR. Evaluation of the setting properties and retention characteristics of mineral trioxide aggregate when used as a furcation perforation repair material. J Endod 1998;24:768 –71.
8. Estrela C, Bammann LL, Estrela CR, Silva RS, Pecora JD. Antimicrobial and chemical study of MTA, Portland cement, calcium hydroxide paste, Sealapex and Dycal. Braz Dent J 2000;11:3–9.
9. Saidon J, He J, Zhu Q, Safavi K, Spangberg LS. Cell and tissue reactions to mineral trioxide aggregate and Portland cement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:483–9.
10. Angelus. MTA Angelus: cimento reparador. Londrina: Angelus.
11. Menezes R, Bramante CM, Letra A, Carvalho VG, Garcia RB. Histologic evaluation of pulpotomies in dog using two types of mineral trioxide aggregate and regular and white Portland cements as wound dressings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:376 –9.
12. Song JS, Mante FK, Romanow WJ, Kim S. Chemical analysis of powder and set forms of Portland cement, gray ProRoot MTA, white ProRoot MTA, and gray MTA-Angelus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:809 –15.
13. Abdullah D, Pitt Ford TR, Papaioannou S, Nicholson J, McDonald F. An evaluation of accelerated Portland cement as a restorative material. Biomaterials 2002;23: 4001–10.
14. De-Deus G, Coutinho-Filho T. The use of white Portland cement as an apical plug in a tooth with a necrotic pulp and wide-open apex: a case report. Int Endod J 2007;40:653– 60.
15. Bortoluzzi EA, Broon NJ, Bramante CM, Garcia RB, de Moraes IG, Bernardineli N. Sealing ability of MTA and radiopaque Portland cement with or without calcium chloride for root end filling. J Endod 2006;32:897–900.
16. Weldon JK, Pashley DH, Loushine RJ, Weller RN, Kimbrourg WF. Sealing ability of mineral trioxide aggregate and super-EBA when used as furcation repair materials: a longitudinal study. J Endod 2002;26:467–70.
17. Camps J, Pashley DH. Reliability of the dye penetration studies. J Endod2003;29:592– 4.
18. Lemon RR. Nonsurgical repair of furcation defects. Internal matrix concept. Dent ClinNorth Am 1992;36:439 –57.
19. Hamad HA, Tordik PA, McClanahan SB. Furcation perforation repair comparing gray and white MTA: a dye extraction study. J Endod 2006;32:337– 40.
20. Bargholz C. Perforation repair with mineral trioxide aggregate: a modified matrix concept. Int Endod J 2005;38:59–69.
21. Lee SJ, Monsef M, Torbinejad M(1993). Sealing ability of a mineral trioxide aggregate for repair of lateralroot perforations. J Endod.;19: 541-544.
22. Islam I, Chng HK, Yap AU. Comparison of the root-end sealing ability of MTA and Portland cement. Aust Endod J 2005;31:59–62.
23. Arens DE, Torabinejad M. Repair of furcal perforations with mineral trioxide aggregate: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:84–8.
24. Song JS, Mante FK, Romanow WJ, Kim S. Chemical analysis of powder and set forms of Portland cement, gray ProRoot MTA, white ProRoot MTA, and gray MTA-Angelus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:809 –15.
25. Islam I, Chng HK, Yap AU. Comparison of the root-end sealing ability of MTA and Portland cement. Aust Endod J 2005;31:59–62.
26. De-Deus G, Petruccelli V, Gurgel-Filho E, Coutinho-Filho T. MTA versus Portland cement as repair material for furcal perforations: a laboratory study using a polymicrobial leakage model. Int Endod J 2006;39:293– 8.
|