INTRODUCTION
The definition of an impacted tooth is “A tooth that cannot erupt into its normal functioning position and is pathologic and therefore require treatment”. The third molars are the most frequent impacted tooth followed by maxillary permanent canines and mandibular second premolars rank 3rd in frequency of order of impaction. The impaction of first permanent molar is extremely rare. Dachi and Howell, 1961 found the incidence of impacted canine in maxilla is 0.92% and of other non-third molar impaction is to be 0.38%. The first permanent molars seem to be impacted more frequently than the second permanent molars.
In most of our review of literatures it was found that impaction of first permanent molars are due to ectopic eruption and it may cause resorption of distal root of deciduous second molars or even premature
exfoliation of the same.
The causes for impaction are both systemic and local. Systemic factors like endocrine deficiency (hypothyroidism and hypopituitarism), febrile disease, irradiation, down’s syndrome and cleidocranial dysostosis may influence impaction of permanent teeth. In all these conditions generally multiple teeth are involved. The local factors which are more commonly involved in permanent tooth impaction are prolonged retention of deciduous tooth, premature loss of primary molars, arch length deficiency, supernumerary tooth, malposed tooth germ, abnormal path of
eruption, trauma and cleft lip and palate. Dentigerous cyst, ankylosis of primary molars, odontomes and supernumerary tooth may be the cause for molar impaction. Raghoebar and Colleague, 1991 stated that impaction of first permanent molar was often diagnosed as ectopic eruption, whereas impaction of second permanent molar is associated with arch length deficiency.
CASE REPORT:
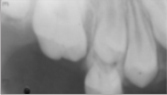
The present case is a 12 year old boy who reported to the department of Pedodontics and Preventive Dentistry at Himachal Dental College, Sundernagar, H.P. with an impacted maxillary permanent first molar (#26). The other three molars were erupted in time and they were well in occlusion. On palpation the impacted molar could not be felt on buccal or lingual position. There was no deficiency of arch length in this present case. The intra-oral periapical radiograph showed vertical position of the impacted tooth with a thick band of mucosa and bone covering the crown of the tooth. The second permanent molars were not erupted and they were well in place i.e. there was no mesial migration of 27 causing impaction of 26. The patient gave a history of an accident at 5 years of age which is reflected through a scar tissue present on his face. There were no other causes for impaction of 26 except that of local trauma. In this present case there was also delayed eruption of tooth # 23, 24 and 25 which were erupting spontaneously.
 |
 |
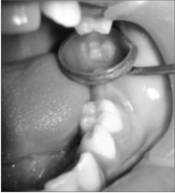
Preoperative Photographs (Extraoral and Intraoral)
On the basis of following diagnosis a decision of surgical exposure of the impacted tooth was made. Prior to surgical procedure routine blood and urine examination were carried out which were within normal limit. The operation was performed under local anesthesia. A circular incision was given in the mucosa around the crown of the impacted tooth to remove the thick band of soft tissue. With a surgical bur the bone above the crown of the impacted tooth was removed along with copious flow of normal saline. When the crown was exposed, it was irrigated with normal saline to remove any bony spicules and debris. The hemorrhage was arrested with pressure pack. The surgical wound was then packed with a coe-pack to prevent epithelization of the crown. It was necessary to change the coe-pack repeatedly after thorough irrigation. The patient was asked to maintain good oral hygiene and a chlorhexidine mouth rinse was prescribed for plaque control.
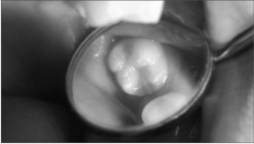
Surgical exposure
Placement of Coe-pack
After 1 month
After 9 months
Routine check up and radiographs were taken after regular interval to assess the improvement of eruption of the tooth. The tooth is now erupted into the oral cavity.
Pre-operative radiograph
After 1 month of surgery
After 6 months of surgery
DISCUSSION:
The management of an impacted tooth often necessitates a complex surgical and orthodontic treatment. In this present case we opted for surgical exposure only and periodic follow up for its eruption. The permanent first molar was impacted for more than six years which made us to opt for surgical exposure as soon as possible. The tooth was spontaneously erupting but very slowly. This is because the erupting force of the tooth was negligible owing to the completion of the root formation. It took 9 months for complete eruption of the tooth in the oral cavity. In this case a light (40gms to 60gms) orthodontic force would have been better for eruption guidance for faster eruption.
Kokich, 1993 described the surgical and orthodontic management of impacted tooth and identifies the position and angulation of the impacted tooth, length of treatment time, space availability and the presence of keratinized gingiva as a critical factors that will affect prognosis and treatment outcome. The cost involved in orthodontic traction for impacted tooth may also influence the type of treatment options. In this present case we did not go for orthodontic traction because the patient would not be able to afford it. Other factors such as patients medical history, dental status, oral hygiene, functional and occlusal relationship, attitude towards orthodontic treatment and compliance with treatment will influence the choice of treatment options.
critical factors that will affect prognosis and treatment outcome. The cost involved in orthodontic traction for impacted tooth may also influence the type of treatment options. In this present case we did not go for orthodontic traction because the patient would not be able to afford it. Other factors such as patients medical history, dental status, oral hygiene, functional and occlusal relationship, attitude towards orthodontic treatment and compliance with treatment will influence the choice of treatment options.
The successful management of an impacted permanent first molar by surgical exposure followed by placement of a coe-pack to maintain the patency of the wound for eruption of the tooth is not new. This case is an unique example because the thick fibrous band of mucosa and bone over the impacted permanent first molar did not allow the tooth to erupt but at the same time the tooth was not ectopically erupting. It was impacted for more than 6 yrs and there was no pathological lesion developed over the crown. If not treated early the corresponding mandibular first permanent molar will passively erupt and it may cause traumatic occlusion later on. There may be development of dentigerous cyst, pre-eruptive caries, periodontal problems or infection from the impacted tooth. Therefore, an impacted permanent first molar should be treated as and when it was diagnosed. Surgical removal of the impacted permanent first molar is indicated where there is no hope for its eruption and when it causes pathological root resorption of the adjacent tooth or when it causes severe arch length deficiency leading to impaction of the second permanent molar. In all circumstances one should try to preserve the permanent first molar for better occlusion and function. Acknowledgement
Dr. Anshul Sachdeva, P.G student 2nd year, to keep all the records of the patient as well as corresponding to the patient in time.
REFERENCES:
1. Dachi SF, Howell FV. A survey of 3,874 routine full mouth radiographs II. A study of impacted teeth. Oral Surg Oral Med Pathol 1961;14:1165-9
2. Raghoebar GM, boering G, Vissink A, Stegenga B. Eruption disturbances of permanent molars: a review. J Oral Pathol Med 1991;20:159-66.
3. Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod 1994;64:249-256.
4. Chaushu S, Sharabi S, Becker A. Dental morphologic characteristics of normal versus delayed developing dentitions with palatally displaced canines. Am J Orthod Dentofacial Orthop 2002;121:339-346.
5. Kokich VG, Methews DP. Surgical and orthodontic management of impacted teeth. Dent Clin North Am 1993;37(2):181-204.
6. Bishara SE. Impacted maxillary canine: a review. Am J Orthod Dentofacial Orthop 1992;101:159-171.
7. Ohman I and Ohman A. The eruption tendency and changes of the direction of impacted teeth following surgical exposure. Oral Surg Oral Med Oral Pathol 1980;49:383-9.
8. McNamara C. and McNamara T. G. Mandibular premolar impaction: 2 case reports. J Can Dent Assoc 2005; 71(11):859-63.
9. Grover PS Lorton L. The incidence of unerupted permanent teeth and clinical cases. Oral Surg Oral Med Oral Pathol 1985; 59: 520-5. |