Introduction:
Approximately 90% of the Orthodontic patients report pain[1], making it the most commonly reported detrimental effect of Orthodontic treatment and the greatest reason for wanting to discontinue or avoid orthodontic care[2]. Despite numerous studies detailing discomfort as a discouraging aspect of Orthodontia[3], it has been noted that both pain and discomfort decrease after third day [1],[4].
For orthodontic treatment with fixed mechanotherapy, separation of teeth is invariably required to place bands, accomplish interproximal stripping, etc. Many studies regarding the separation effect have been undertaken, but, few have evaluated the patients’ perception of the pain and discomfort related to the same[5]. The aim of this study was to examine three types of orthodontic separators, (elastomerics, Kesling’s wire separators and brass wire separators) focusing on the patients’ perception of pain and discomfort.
One of the biggest problems in assessing pain is that it is subjective. Many scales and scores have been devised to assess pain like visual analogue scale (VAS), McGill’s questionnaire etc.[6],[7]. By far the most popular scale is VAS. It contains digits from 1 to 10. The person is asked to compare the severity of current pain when compared to worst pain he has ever faced in life (like labour pain, surgical pain, fracture pain). Having known the current pain at the beginning of the treatment, when patient comes for follow up, the pain relief can be assessed by asking him to compare his pre-treatment pain with post-treatment one[8]. By far, this is the easiest5 both to administer and score, and also is the simplest type[8] as shown in Fig. 1.
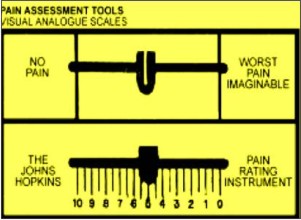 | Fig.1: Types of Visual analogue scales
 |
Materials and Method:
90 patients, 45 boys and 45 girls, aged between 15-18y (mean age: 16.7y), none of whom had undergone an orthodontic treatment earlier, participated in the study. To be included in the study, they had to sign an informed consent and undergo fixed orthodontic mechanotherapy. They were explained that the procedure was a part of their treatment. At baseline, i.e., on the day of the procedure, prior to separator placement, any dental pain was ruled out while chewing. The three types of separators used were:
(a) elastomeric separators
(b) Kesling’s wire separators, and
(c) brass wire separators.
These were placed mesial and distal to the permanent first molars as shown in figures 2 through 4. The perception of pain and discomfort was then assessed by a questionnaire (attached alongwith) and visual analogue scale over a period of four days, when the patient was recalled for removal of separators and placement of bands.
 | Fig 2: Elastomeric separators
|
 | Fig 3: Kesling’s separators
|
 | Fig 4: Brass wire separators
|
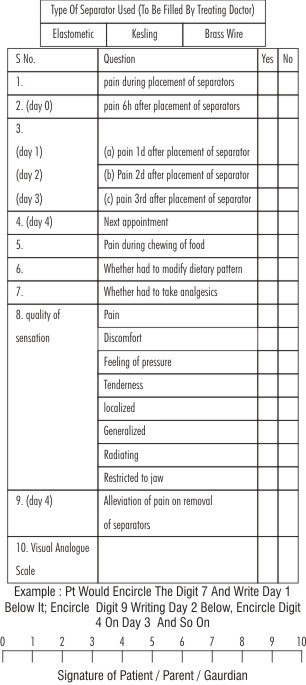 | Questionnaire Used
|
Results:
All 90 patients completed the study. Response rate was excellent since all patients responded to all questions on all questionnaires. The baseline survey before separator placement revealed that none of the patients had any pain from the molars at rest or even while chewing.
More number of patients in the group with brass separators perceived pain as compared to the other two groups, i.e., Kesling’s wire separators and elastomeric separators (p value E/K 0.0575*, p value E/B 0.2857, p value K/B 0.0032**).
62 of the ninety patients were in such severe pain that they needed analgesics to relieve it (P < .05), and significantly more girls than boys had used analgesics (P < .05). 75 patients had to change their food habits (P < .05) and this also applied to significantly more girls than boys (P < .05).
Discussion:
It was found that mild to moderate pain was associated with the separators. Brass wire separators caused most pain and discomfort. The pain was perceived as worst at day 2 while it subsided almost completely by day 4. The varying degree of individual pain/discomfort response to application of orthodontic forces has previously been reported[4],[9] as established in this study also.
Another important predictor of pain is gender[10],[11] In this study, no significant difference was found between boys’ and girls’ pain discomfort experience during the separation. Although a few studies have claimed that girls report more pain / discomfort than boys[1],[12], the literature seldom points to any correlation between gender and perception of pain / discomfort during orthodontic treatment[1],[4],[9]. Nevertheless, in this study, it was found that significantly more girls (37) than boys (25) had used analgesics in spite of similar perception of pain. It has been reported earlier that orthodontic patients use analgesics fairly often[1],[5].
Among daily activities, eating was most affected during the separation period, and the influence on food choices was reasonably considerable, since 75 of 90 patients had changed the dietary pattern to soft food. These findings are in accordance with other previous studies[1],[5].
VAS (Visual Analogue Scale) was used considering its simplicity[1],[5] and lack of failures under the age of 5y[13]. It has also been found that VAS is a useful tool when patients have to discriminate between pain / discomfort in the posterior and anterior teeth after initial placement of an archwire[14]. Bondemark et al found that patients had no problems in discriminating between pain / discomfort between right and left posterior teeth when two different separators were placed between right and left side, respectively[5].
Conclusion:
All the three types of separators caused pain of mild to moderate intensity with elastomeric and Kesling wire separators considered less painful than the brass ones, though the difference was not statistically significant. Pain was worst after 2 days and had almost completely subsided by day 4. Therefore, molar band placement should be done at least 4 days after separator insertion. Also, analgesics and soft food must be recommended for patients’ comfort.
References:
1. Scheurer P, Firestone A, Burgin W. Perception of pain as a result of Orthodontic treatment with fixed appliances. Eur J Orthod. 1996;18:349-357.
2. Oliver R, Knapman YM. Attitudes to Orthodontic treatment. Br J Orthod. 1985;12:179-188.
3. Tayer B, Burek M. A survey of adult’s attitudes toward Orthodontic therapy. Am J Orthod Dentofacial Orthop. 1981;79:305-315.
4. Jones ML. An investigation into the initial discomfort caused by placement of an archwire. Eur J Orthod. 1984;6:48-54.
5. Bondemark L, Fredriksson K, Ilros S. Separation effect and perception of pain and discomfort from two types of Orthodontic separators. World J Orthod 2004;5:172-176.
6. Muralidhar Joshi. Clinical history. In Textbook of Pain Management; Muralidhar Joshi, 1st ed, Paras Publishing: 2005;7; 30-35.
7. Melzack R. The McGill Pain Questionnaire; Major properties & society methods. Pain, 1975; 1; 277-279.
8. Dr. Muralidhar Joshi. Evaluation of pain. Indian J Anaesth2006;50(5):335 – 339.
9. Fernandes LM, Ogaard B, Skoglund L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. J Orofac Orthop1998;59:331-339.
10. Riley JL, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex differences in the perception of noxious experimental stimuli: A meta analysis. Pain 1998;74:181-187.
11. Bergius M, Kiliaridis S, Berggren U. Pain in orthodontics. A discussion and review of literature. J Orofac Orthop 2000;61:125-137.
12. Kvam E, Gjerdete NR, Bondevik O. Traumatic ulcers and pain during Orthodontic treatment. Community Dent Oral Epidemiol 1987;15:104-107.
13. Scott J, Ansell BM, Huskisson EC. The measurement of pain in juvenile chronic polyarthritis. Ann Rheum Dis 1977;36:186-187.
14. Ngan P, Kess B, Wilson S. Perception of discomfort by patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop 1989;96:47-53.
|