Introduction:
Every human in this world wants to lead a healthy life. The amount of well being which an individual enjoys is governed by the standard of living which includes income, occupation, and sanitation, and education, level of provision of health, recreation and nutrition.[1]
Throughout life, nutrition andoral health are interdependent. Nutrition plays two quite different roles in oral healthi.e.protective and preventive. The preventive effect of food has been recognized since the 18th century when James Lind advocated the intake of fresh fruits and vegetables for the prevention of scurvy.[1]
Apples, pears, mango, banana and cantaloupe are all examples of fibrous fruits and can have a benificial effect on both general and oral health.[2] Apples have been regarded as nature’s tooth brush as they are likely to contain condensed tannins which have anti-adhesion properties that may help prevent periodontal or gum disease because they inhibit some bacteria from bonding to each other and producing dental plaque.[3]
Most of the farmers and migrant workers help in the harvesting of apples during the picking season in Himachal Pradesh, as its geographical location favors its cultivation.[4],[5] Despite the fact that they help reach apples in different parts of the country, they remain one of the poorest, most economically disadvantaged working people throughout the world. Inspite of being struck with Poverty and not having access to information that could prevent oral health problems, these farmers might still be seen with good oral hygiene. This could be due to the fact that they consume a lot of apples during the picking season.[6]
Till date very few studies are available on the oral health status of the farmers working in apple orchards and the literature available on the other farm workers in different parts of the world show high level of untreated dental caries, missing teeth and gingivitis.[6] Hence this study was taken up to assess the oral health status and the treatment needs of farmers working in the apple orchards of Shimla.
Materials And Methods:
After getting the ethical clearance from review board of The Oxford College and permission from Panchayat or village head and owner of the orchards a pilot study was conducted to estimate the sample size and to identify any organizational and technical problems
The sample size was derived with the help of the following formula:
n= {2alpha + 2(1-beta)}2 pq
---------------------------
E2
If p= 18%, q= 82, E=3.6, then by applying the above formula, the sample size was 892. This was rounded of to 900. Himachal Pradesh has a total of 113357 apple orchids, out of which 44251 are in Shimla. As each orchard had 2 permanent workers, 450 apple orchards were selected.
Before the start of the study, the investigator was standardized and calibrated in the department of Public Health Dentistry, first by practicing the on a group of 10 subjects with a the full range of conditions expected to be assessed in the survey The result so obtained was subjected to kappa statistics. The Kappa co-efficient value (0. 80) showed substantial agreement for intra-examiner reliability.
The subjects who were permanent workers in the orchards and gave consent were invited to take part in the study. The farmers who were suffering from systemic problem or were under medication which could affect the oral health were excluded from the study. The data was collected with help of specially prepared proforma (demographic details, personal habits, oral hygiene, dietary practices and plaque index by Silness P.and Loe H.) and WHO 1997 proforma.
The study was systematically scheduled to spread over a period of 2 month. A weekly and monthly schedule was prepared well in advance and on an average 20 subjects were examined per day
The examination was carried under natural light in the apple orchards with the subjects sitting comfortably on an ordinary chair with back rest and with the examiner standing behind or at the side of the chair. The recorder was made to sit close to the examiner so that instructions and codes could be easily heard and the examiner could see that the findings were being recorded correctly. Any dental observations requiring treatment were informed to the subjects and proper disinfection of the instruments were done after clinical examination.
Statistical Procedure:
Analysis of the data was done according to the guidelines given by WHO oral health surveys, basic methods. Descriptive statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ±SD and results on categorical measurements are presented in Number (%). The Statistical software namely SPSS 15.0, Stata 8.0, MedCalc 9.0.1 and Systat 11.0 were used for the analysis of the data.Microsoft word and Excel have been used to generate graphs, tables etc.
Result:
The total study population was 900, comprising of 660 males and 240 females in the age group of 18-80 years with the mean age of 41.91± 12.94.
64 subjects (7.1%) belonged to lower and 836 (92.9%) belonged to upper lower socioeconomic class.
Out of the total population around 399 subjects (44.3%) had visited the dentist and 501 subjects (55.7%) had never visited a dentist.
The number and percentage of subjects with healthy oral mucosa were found to be 794 (88.2%); subjects with leukoplakia were found to be 80(8.8%), ulceration 15(1.6%) and 11(1.2%) other condition. Leukoplakia was mainly found on the buccal mucosa with one having on the hard palate.
The mean number of sextant with healthy periodontal tissue was found to be 0.25 ± 0.95, that of bleeding 0.28 ± 0.90, calculus 4.69 ± 1.99, shallow pockets (4-5mm) 0.31 ± 0.63 and deep pockets (> 6mm) 0.02 ± 0.15.
The mean number of sextant with the loss of attachment by score is as follows: loss of attachment 0-3 mm was 4.99 ± 1.88, 4-5mm was 0.34 ± 0.8, 6-8mm was 0.04+ 0.25 and 9-11mm was 0.001± 0.03.
The mean number of decayed permanent teeth per person was 5.01 ± 3.31. The mean number of filled and missing permanent teeth per person was 1.48 ± 2.95 and 0.03 ± 0.26.
Treatment needs among workers showed that 31.9% of the subjects needed one surface filling, 12.4% of the subjects needed two surface filling, 4.4% of the subjects needed pulp care and restoration 9.6% of the subjects needed extraction and 40.4% of the subjects needed some other care.
Number and percentage of subjects requiring prosthesis, by type of prosthesis and by jaw shows that 119 (13.2%) and 105(11.6%) needed one unit prosthesis, 141(15.6%) and 121(13.4%) needed multi unit prosthesis, 49(5.4%) and 40(4.4%) needed a combination of one or multiple prosthesis and 35(3.8%) and 33(3.6%) needed full prosthesis in the upper and lower jaw respectively.
Percentage of subjects with crowding, spacing, and diastema 9.4 %, 6.1 %, 3.0 % and anterior maxillary or mandibular irregularities was, 8.6% and 6.0% respectively 85% of the subjects had no abnormality or minor malocclusion, which need no or slight treatment .
The information regarding their usage of oral hygiene aids showed that 88.5% of the subjects cleaned their teeth with the help of toothbrush and dentifrice. 5.6% used to clean their teeth with finger and walnut leaves or tooth powder while 5.9% used to clean it with timber stick.
Subjects with good oral hygiene recorded low CPI scores and comparatively less loss of attachment Figure 1 represents the loss of attachment according to the frequency of cleaning.
The plaque scores of the whole group was 0.9, which was a good score. Figure 2 shows the distribution of the population according to the plaque score
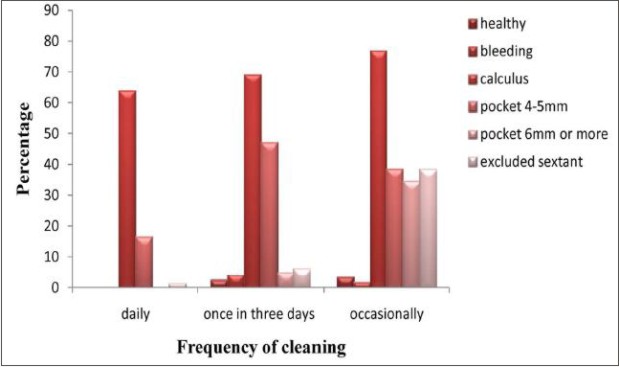 | Figure 1: Distribution Of Study Population According To CPI And Frequency Of Cleaning
 |
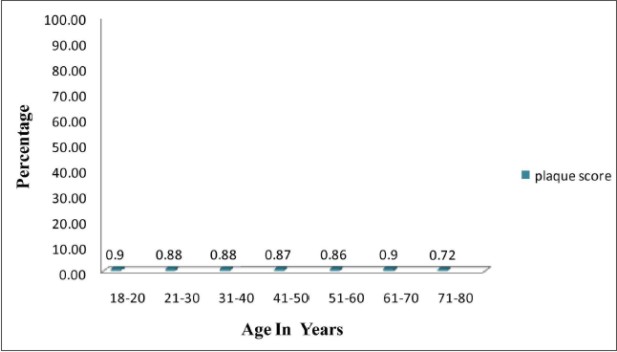 | Figure 2: Distribution Of Population According To Plaque Score
|
Persons who use to brush their teeth daily had a mean DMFT score of 5.32 ± 3.93 and the persons who used to brush the teeth once in three days and occasionally had mean DMFT score of 10.27 ± 5.90 and 17.12 ± 8.47.
The prevalence of caries with respect to the consumption of apples is presented in Table 1. It was seen that the prevalence of caries increased as the consumption of apples increased per day.
The prevalence of leukoplakia showed a linear relationship with the duration and frequency of the use of smoking tobacco. Table 2 and 3 presents the distribution of study population having leukoplakia along with the usage of tobacco products.
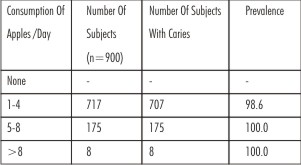 | Table 1: Distribution Of Study Population According To Of Prevalence Of Caries And Consumptionof Apples Per Day During Picking Season
|
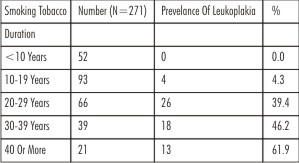 | Table 2: Distribution Of Study Population According To Prevalence Of Leukoplakia And Duration Of Use Of Tobacco Products
|
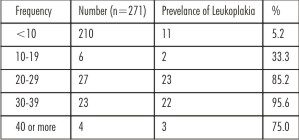 | Table 3: Distribution Of Study Population According To Prevalance Of Leukoplakia With Frequency Of Tobacco Products
|
Discussion:
Apples are one of the most popular fruits in the world. Almost 92000 hectares of land in the state Himachal Pradesh) is under apple production, producing 40,000 metric tonesapples per year and involving 80% of the people in the state directly or indirectly with this business In spite the hard work the apple farm workers put to cultivate them, they remain the most disadvantage group due to there low wages. Upon this they have very limited access to the health services which make them a highly vulnerable to various diseases.
Till date very few studies are available on the oral health status of the farm workers working in apple orchards, so the present study was compared with the available literature and data available from the National Oral Health Survey & Fluoride mapping 2002-2003 of Himachal Pradesh State (Rural)
Out of the total sample 55.7% had never visited the dentist. They made the minimal utilization of Preventive services and health education and visited the dentist only in case of emergency. This result was similar to the study conducted by George M. in the Puerto Rican migrant workers.[7] The various obstacles which prevented them to seek dental care were availability of appointments, transportation.
The study population used to consume 1-8 apples during the picking season, which was similar to the study conducted by the South Africian researchers amongst the apple, grape and grain farm workers. They were seen to consume around 8 apples and 8 bunch of grapes daily during the picking season.[9]
Timber sticks and walnut leaves were mostly used by the old people, while the tooth brush and paste were used by the younger generation. This showed that there is a tremendous increase in the modernization of the rural people who are leaving their traditional ways to just move with the society.
Concerning the prevalence of leukoplakia, 80 subjects had leukoplakia on the buccal mucosa and 1 person had it on the hard palate. The subjects who had signs of leukoplakia used to consume large amount of tobacco in form of cigarette and bidi. But interestingly no body in the study population showed any signs of oral cancer. This may be due to the fact that Quercetine in apples help to reduce the risk of cancer. This finding is in contrast to the findings observed in the National Oral Health survey conducted in the year 2002 were 2% of the subjects in the age group of 65- 74 years had oral cancer.[8]
The present study shows that 73.4% of the male had various form of periodontal disease as compared to 98.8% in females. These findings were different from the results recorded by Bagramin RA in Amish population were men had high prevalence of periodontal disease.[10]
In the present study only 65.4% of the subjects had calculus which was comparatively low when compared to the study conducted by Bagramin RA, where 84% of the subjects had calculus.[10] This finding was also less when compared to the National Oral Health Survey conducted in Himachal Pradesh, where 89.9% of the subjects had calculus.[8]
When the pocket depth were recorded it was seen that 22.4 % of the subjects had 4-5mm pocket depth 2.0% of the subjects had pocket depth upto 6 mm or more. This findings were comparatively low when compared to the study conducted by Bagramian RA in an Amish population were 97% of the Amish had pocket depth equal to or greater than 4 mm and 27% of the subjects had pocket depth about 6mm and more.[27]. The various pocket depths recordings in the present study was also less when compared to the National Oral Health Survey, 39.3% of the subjects had 4-5mm pocket depth and 28.0% of the subjects had pocket depth upto 6 mm or more.[8].
In the present study 18.8% subjects had 4-5 mm loss of attachment and 3.3% subjects had 6- 8 mm loss of attachment. These findings were comparatively less when compared to the study done by Bagramian RA. They reported that 57.1% of the subjects had 4mm or greater loss of attachment and 16.7% of the subjects had 6mm or greater attachment loss.[9]
When the mean DMFT scores of the present study was compared with the other studies, it was seen that the total mean DMFT of the present study was 6.51± 5.21 which was comparatively less than the studies conducted by George M. in the Puerto Rican migrant workers[7] and by Grobler SR in apples or grapes workers9. The former study recorded a mean DMFT score of 54.8 and the latter recoded a mean DMFT score of 24.2 in the apple group, 17.4 in the grapes group and 9.9 in the control group.
The prevalence of dental caries in the present study population was 98.9%. The subjects who used to consume around 5-8 apples or more than 8 apples per day during picking season exhibited 100% prevalence. The subjects who never consumed sweets or used to consume fewer amounts of sweets also showed high prevalence of about 88.4% and 97.1%. This could be due to the fact that apples have high sugar content, despite being good for periodontal condition
The subjects in the present study recorded high unmet treatment needs which was in accordance to the study conducted by GeorgeM. in the Puerto Rican migrant workers.[7]
The plaque score of the subjects participating in the study was 0.9. This finding is in accordance to the study conducted in the Amish workers were 30% of teeth didn’t had plaque.[10] The less plaque score in the present study was due to the fact that the study was conducted at the time of the picking season during which they consumed high numbers of apples which are believed to inhibit plaque formation. The fact that apples have intrinsic sugar and consumption of these and dental caries was proportional. In this view also further research is required.
As plaque plays a crucial role in the development of periodontal problems, we can derive at a hypothesis that apples are beneficial for periodontal health but this requires further studies to be carried out for finding out the exact association of the variables.
Conclusion:
The less plaque scores may be due to inhibition of plaque formation due to consumption of the apples just during the picking season. As apples are available to them just during the picking season and they have poor oral hygiene further research on the beneficial effect of apples needed to be carried out. This study also brought to notice the high demand of treatment need amongst the population. Further research is required to get the insight of the cultural practices and taboos related to oral health and practices prevalent among the farmers. Hence a program to increase the presence of appropriate dental personal in the remote villages to implement educational and preventive dental programmes and improvement in the physical infrastructure in the remote villages offer the best opportunity for improving the oral health of the farmers
References
1. K Park. Park’s textbook of Preventive and Social Medicine. 19th edition,Banarsidas Bhanot Publication, 2007
2. URL: http://www.mydigitalfc.com/knowledge/healing-power-fruits-555
3. URL: http://www.bcfga.com/index.php?sectionID=4&pageID=16
4. URL:http://www.thaindian.com/newsportal/business/rain-snow-cheer-apple-growers-in-himachal-pradesh_100175023.html
5. URL: http://www.livemint.com/2008/05/30000151/Rains-hit-Himachal8217s-app.html
6. Daniel Hawkins, Gina R. Lombardi. Migrant Health Issues- Monograph Series, 1-57
7. George M.Gluck, Charles D. Knox. Dental Health of Puerto Rican Migrant Workers. Health Services Reports 1972; 87; 456-460.
8. WHO. National Oral health Survey and Fluoride Mapping 2002-2003. Dental Council Of India
9. S.R.Grobler,J.B.Blignaut. Dental effects of apples and grapes. Nutrition Research Newsletter 1989.
10. Bagramian RA, Farghaly MM, Lopatin D, Sowers MF. Periodontal disease in an Amish population. J Cliin Periodontol 1993;20;269-272
|