Introduction
Impaction of Maxillary Permanent incisor is not a common occurrence in dental practice but when present, it can have a major impact on dental and facial esthetics. It is regarded as unattractive and may affect the self esteem and general social interaction of the child. Therefore, it is important to diagnose and manage the problem as early as possible. Fortunately parental concern regarding the delay in eruption of maxillary central incisor facilitates early diagnosis of the problem in mixed dentition stage.
The most common causes of impaction of permanent maxillary incisor are presence of supernumerary teeth and trauma to primary dentition. It has been reported that 50-60% of supernumerary teeth cause impaction of permanent incisors.[1] The less common causes include retained primary teeth, presence of mucosal or bony barriers, abnormal developmental position and or angulation of root and presence of odontogenic cysts and tumours.
Removal of supernumerary tooth leads to spontaneous eruption of impacted maxillary incisors in 54-70% of cases[2],[3],[4],[5] provided there’s adequate space in the arch, however, the research indicates that the process of spontaneous eruption may take upto 3 years and may not occur at all in many cases. It is therefore necessary in such cases to carry out a surgical exposure of the impacted maxillary incisor by removing any hard or soft tissue obstruction, placement of attachment on the tooth crown followed by orthodontic traction of the impacted tooth into proper alignment.[4],[5],[6],[7]
The present article reports two cases of maxillary central incisor impactions, one of which is secondary to presence of supernumerary tooth.
Case - I
A 10 year old boy reported to the department of Paedodontics & Preventive dentistry, D.A.V (C) Dental College & Hospital Yamuna Nagar, Haryana. The chief complaint was non-eruption of upper right central incisor. The child was physically healthy and had no history of medical and dental trauma.
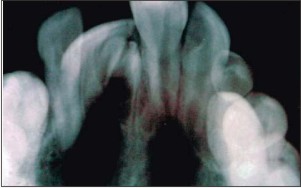
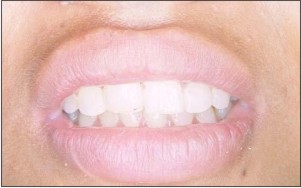
Clinical examination revealed an early mixed dentition stage and a Class-I molar relationship. A bulge in the labial sulcus with no apparent arch-length discrepancy was noticed.(Fig 1) An intraoral periapical radiograph revealed a supernumerary tooth in the vicinity of maxillary right central incisor causing its impactionAn upper anterior occlusal radiograph was taken to confirm the position of supernumerary tooth on the buccal aspect. (Fig 2) It was decided to extract the supernumerary tooth followed by surgical exposure of the impacted tooth and pull it down to its normal position in the arch with the help of orthodontic traction. Treatment was explained to the patient & his parents and consent was obtained.
For the procedure local anaesthetic was administered and gingival was excised in the involved area. Adequate amount of bone was removed with rotary cutting instruments to expose the supernumerary tooth. The tooth was removed(Fig 3) and surgical exposure of the permanent central incisor was carried out by removing 4-5mm of bone from the most superficial portion of the labial aspect of the anatomic crown.(Fig 4) Care was taken to maintain 2-3mm of keratinised tissue over the CEJ. An orthodontic bracket was bonded to the exposed part of the crown. An orthodontic appliance was bonded to all teeth in maxilla. The impacted tooth was ligated to a 0.016 round wire with the help of ligature wire. Patient was recalled after 2 weeks.(Fig 5)
Orthodontic traction of impacted central incisor was continued till it achieved proper alignment in the arch. (Fig 6) Acceptable gingival contour and attached gingival was found in the aligned CI, three months post operatively.(Fig 7)
Case - 2
A 12 year old girl reported to the department of Paedodontics & Preventive dentistry, D.A.V (C) Dental College & Hospital Yamuna Nagar with the chief complain of unerupted right maxillary central injcisor. The child was physically healthy and had no other significant medical history. Patient gave no history of dental trauma. History regarding over-retained primary tooth was unclear.
Clinically a bulge was seen in the labial gingival on the right maxillary central incisor.(Fig 2.1) The tooth was positioned high up in the alveolar bone with a thick layer of bone covering the tooth. The space in the maxillary arch needed for proper alignment of impacted central incisor was found to be inadequate.
The treatment plan included to regain the space for unerupted central incisor by placing an orthodontic appliance in the maxillary arch and then surgically expose the impacted central incisor by removal of gingiva and bone overlying the crown of the impacted tooth. (Fig 2.2) The tooth was then guided into occlusion by orthodontic traction. (Fig 2.3) Patient was recalled at a periodic interval of 2 weeks till the tooth came into proper alignment. (Fig 2.4)
 | Figure 1
 |
 | Figure 2
|
 | Figure 3
|
 | Figure 4
|
 | Figure 5
|
 | Figure 6
|
 | Figure 7
|
 | Figure 2.1
|
 | Figure 2.2
|
 | Figure 2.3
|
 | Figure 2.4
|
Discussion
Treatment of impacted maxillary incisors is challenging because of their importance to facial esthetics. Etiology behind impaction of these teeth may be related to abnormal developmental position of tooth, retained deciduous teeth and various cysts and tumours. Supernumerary teeth are the most common cause of impaction of maxillary incisors.[8]
The treatment of impacted maxillary incisor depends on its state, position and the space present in the dental arch.[9] It is of utmost importance that central incisors take their correct position in the dental arch as soon as possible because of their prime importance in esthetics and alignment in anterior segment.
Though research indicates that impacted incisors may erupt spontaneously after removal of the supernumerary teeth but it may take 2-3 years of time.[5] In some instances, the tooth simply fails to erupt. It has been reported that 36.4% of impacted maxillary incisors fail to erupt on their own.[4],[10]
The strategic location of maxillary central incisors makes it mandatory that they take their right position in the arch as soon as possible to avoid esthetic & orthodontic problems. Early intervention is the key to successful alignment of anterior teeth in such patients as younger the age, quicker will be the eruption of tooth.[11] Surgical exposure of impacted maxillary incisor and its alignment by orthodontic traction is a well reported procedure in the literature.[12],[13],[14],[15] In the present case report of two cases similar treatment modality was used.
The position and direction of impacted teeth, the degree of root completion and the presence of adequate space for impacted tooth were considered before planning treatment for these cases.
A conservative surgical exposure of the crowns of impacted incisors was carried out in both the cases, leaving 2-3mm of keratinized gingival tissue over the CEJ to prevent gingival recession. This was done in accordance to procedure recommended by Samir E.[16],[17] It has been reported that failure to leave 2-3mm of keratinized tissue over the erupting tooth, leads to significant loss of attachment resulting in recession.
In the second case, space required for proper alignment of central incisor was insufficient. Therefore, the lost space was regained by applying orthodontic forces before the impacted tooth was pulled into alignment. In both the cases the impacted maxillary central incisors could be brought into their normal position within 3 months of orthodontic traction and showed acceptable gingival contour and attached gingival.
Conclusion
Impaction of Maxillary central incisor is a rare finding that can cause significant effect on esthetics and proper alignment of teeth. The key to proper treatment is early diagnosis and intervention.
References:
1. Gregg TA, Kinirons MJ. The effect of the position and orientation of unerupted premaxillary supernumerary teeth on eruption and displacement of permanent incisors. Int J Paediatr Dent 1991; 1: 3-7.
2. Crawford LB. Impacted maxillary central incisor in mixed dentition treatment, Am J Orthod Dentofac Orthop 1997; 112(1): 1-7.
3. Garvey M.T., Barry H.J., Blake M. Supernumerary teeth – an overview of classification, diagnosis and management. J Canad Dent Assoc 1999; 65: 612-6.
4. Mitchell L., Bennett T.G. Supernumerary teeth causing delayed eruption. Br J Orthod 1992; 19: 41-6.
5. Witsenburg B, Boering G, Witsenburg B. Eruption of permanent impacted incisor after removal of supernumerary teeth. Int J Oral Surg 1981: 10: 423-31.
6. Mason C., Azam N., Holt R.D., Rule D.C. A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J Oral Maxillofac Surg 2000; 38: 62-5.
7. Becker A. Early treatment for maxillary central incisors. Am J Orthod Dentofac Orthop 2002; 121(6): 586.
8. Dalia smailiene. Impaction of the central maxillary incisor associated with supernumerary teeth: Initial position and spontaneous eruption timing. Stomatologija, Baltic Dental and Maxillofacial Journal 2006; 8: 103-107.
9. Ibricevic H, Al-Mesad S, Mustagrudic D, Al-Zohejry N. Supernumerary teeth causing impaction of maxillary incisors: Consideration of treatment. J Clin Pediatr Dent 2003;27: 327-32.
10. Housten WJB. A textbook of Orthodontics. 2nd edition. Oxford: Blackwell Sci Publ.; 1995
11. Brin I, Zilberman Y, Azaz B. The unerupted maxillary central incisor: review of its etiology and treatment. ASDC J Dent Child 1982;49:352-56
12. Lin YT. Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofacial Orthop 1999; 115: 406-9.
13. Wassertein A, Tzur B, Breznaik N. Incomplete canine transposition and maxillary central incisor impaction: A case report. Am J Othod Dentofacial Orthop 1997; 111: 635-9.
14. Kolokithas G, Karakakis D. Orthodontic movement of dilacerated maxillary central incisor. Am J Orthod 1979; 76:310-5.
15. Tanaka E, Watanabe M, Nagaoka K, Yamaguchi K, Tann K. Orthodontic traction of an impacted maxillary central incisor. J Clin Orthod 2001; 35: 375-8.
16. Samir E. Bishara. Impacted maxillary canines: A review, 1997 AJO-DO: 1992. P. 159-71.
17. Uematsu S, Uematsu F, Furusawa K, Daguchi T, Kurihara S. Orthodontic treatment of an impacted dilacerated maxillary central incisor combined with surgical exposure and Apicoectomy. The Angle Orthodontist, March 2003; 74(1):132-136.
|