Introduction
Odontogenic developmental anomalies are more frequently observed in primary dentition than in permanent dentition during routine intraoral examination. These variations can be numerical ( hypodontia or hyperdontia) , in tooth structure (size or shape) , eruption wise (early or delayed), or a combination of these because of enamel and dentin malformation.[1],[2] Among the variations of tooth structure anomaly, co-joined teeth are most common. It has been described in several different terms, such as Fusion, Gemination, Double teeth , Twinning, Connation of teeth, syndontia and Conjoined teeth. This occurs more frequently in the mandibular incisors region than the maxillay dentition. Incidence of this anomaly is approximately 0.1% in the permanent and 0.5% in the primary dentition[3].
The tooth bud is made up of cells derived from the ectoderm of the first brachial arch and the ectomesenchyme of the neural crest[4]. Conjoined anomalies or Twinning come under developmental anomalies of proliferation stage.[1] These can be attributed to physical pressure leading to the union of teeth[5] or genetic inheritance[6] as possible etiologies. It is suggested to be caused by the persistence of dental lamina between two or more tooth germs, or by the attempt of a supernumerary tooth to develop from the remnants of the dental lamina after it has divided from a neighboring tooth germ[6]. Since the developmental stage of the buds involved may vary, different clinical and radiographic appearances of these teeth can be found[7].
The most common problem related to fused teeth is hypodontia of the permanent dentition which has been reported in 50% of affected subjects[8],[9],[10],[11].Therefore, early diagnosis of the anomaly is of considerable importance.
The aim of this article is to present 2 cases of unilateral Co-Joining of two primary mandibular teeth - lateral incisor & canine and central & lateral incisors along with assessment of the presence of any associated pathology.
Case Repots:
Case No 1.
A 4 year-old boy reported to the Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences ,Paonta Sahib with chief complain of cavities. Medical history was non remarkable. The mother reported no medications, illnesses, or complications during pregnancy. There was no history of trauma in oro-facial region. Family history and check up was negative to familial tendency to fused teeth showing no unusual findings.
Intraoral examination revealed complete deciduous dentition. The teeth present were 55, 54, 53, 52, 51, 61, 62, 63, 64, 65, 75, 74, 73, 72, 71, 81, x, 83, 84, 85. Out of these,51, 52, 54,55,64 and 84 were carious. 82 was missing.
The intra oral periapical radiograph of mandibular right anterior region showed the following characteristics:
Primary right central incisor and lateral incisors were fused.
Two separate pulp chambers and root canals were present.
The roots of fused primary teeth had just started resorption.
All permanent tooth buds were present confirming no anodontia of permanent dentition.
Case No, 2.
A 10 year old girl came to Department of Pedodontics and Preventive Dentistry, Himachal Institute of Dental Sciences ,Paonta Sahib for examination of extra wide unsightly tooth. No relevant dental, medical and family history was reported. Intraoral examination revealed mixed dentition. The teeth present were 16, 55, 54, 53, 52, 51, 61, 62, 63, 64, 65, 26, 36, 75, 74, 73, 32, 31, 41, x, 83, 84, 85, 46. 42 was missing.
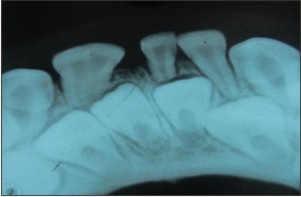
The IOPA radiograph of mandibular right anterior region showed the following characteristics:
Primary mandibular right canine and lateral incisors were fused.
Two separate pulp chambers and root canals were present.
The roots of fused primary teeth had started resorption.
Permanent tooth bud of 42 was missing confirming partial anodontia of permanent dentition.
Informed consent was obtained from the parents of both the patients before any findings were reported.
Discussion
Although there is ample literature on co-joined teeth , there is still much questioning on the nomenclature. Some authors have tried to differentiate these teeth by counting the number or by observing the root morphology. While some use fusion and gemination as synonyms. Some authors call it as “Double teeth” or “connated teeth” to avoid the confusion.[12]
Fusion is often confused with the process of gemination. Gemination occurs when, during the proliferative stage of dental development, a single tooth germ attempts to divide by invagination. These two can be differentiated by the below parameters:[13]
Morphology: Gemination results in mirror images of the coronal halves, whereas fusion takes place at an angle causing a crooked appearance.
Anatomy: Pulpal anatomy is very useful in diagnosing the type of double teeth. Fused teeth would mostly have separate pulp chamber and root canals while geminated usually have one big pulp canal.
Location by jaw: Fusion is common in mandible and gemination in maxilla but fusion between supernumerary and normal tooth is more common in maxilla. Teeth usually have one big pulp canal.
Crowding: Fused teeth would more often cause ectopic eruption and geminated teeth would cause more of crowding. However, when a normal tooth is fused with a supernumerary tooth, crowding and even impaction of other teeth may result. So this factor is not a good diagnostic feature.
Number of teeth: Fusion is counted as one tooth and thus diminishes the number of teeth
whereas number is increased in gemination. According to Mader[14], the ‘two tooth rule’ may be helpful in differentiating fusion from gemination. If the resulting dental structure is counted as two teeth and the normal number of teeth are present in the region, the case probably represents an example of fusion. If, however, the abnormal dental structure is counted as two teeth and if an extra tooth is present in the region, then the case may represent an example of gemination or fusion between a normal and a supernumerary tooth.
Based on the above criteria, our both cases are more inclined towards fusion. Though involvement of supernumerary tooth and anodontia cannot be ruled out clinically or radio graphically.
Fusion can be classified into two types : Complete and Incomplete. Complete fusion starts before calcification of tooth and crown include features of both participating teeth in all the dental tissues as enamel, dentin, cementum and pulp, whereas Incomplete fusion begins at a later stage. In this case, variance in form of separate crowns and limited fusion of roots alone with pulp canals fused or separate.
When fusion occurs, the clinician must be aware of following major dental concerns.
First, since fused teeth are clearly wider, esthetics may be a concern. In our 1st case, the esthetic view was not a problem in the primary dentition and the family was not knowing of the fused teeth until the patient visited dental office. But esthetics was a great concern with our 2nd case of a young girl who has involvement of mandibular right primary lateral incisor and canine , with complete union of the crowns.
Second, when normal teeth fuse, excess dental space can result. This was rather good in our both cases. In the 1st case excess space would be used up by the presence of all permanent teeth whereas in 2nd case anodontia of 42 saves the concern of space.
Third concern relates to both esthetic and occlusion because of unerupted permanent anterior. This is the major concern for patient and parents. When fusion occurs in the primary dentition sometimes it may cause delayed eruption of permanent teeth. The parent counseling was done regarding this subject.
The final concern involves that the surface contour of fused teeth commonly exhibit labial and lingual grooves running vertically on the crown surface. These grooves are very pronounced in cases of incomplete fusion and are difficult to clean and considered to be caries prone zone [15].
In the presented cases, there was a complete fusion. Although grooves were present on the teeth surface no caries was detected at the time of examination. Periodic clinical follow-up was also advised to prevent caries, to check the erupting status of permanent teeth and to allow early intervention whenever pulp alterations and fractures occur.
Treatment of a fused tooth will depend on the clinical situation.
Conclusion
Co - joined teeth like fusion and germination are asymptomatic but both can result in a number of difficulties including tooth reduction in the permanent successors, increased susceptibly to sub gingival bacterial plaque, aplasia or malformation of the permanent successors and impaction. The potential clinical problems associated
with fusion require Orthodontic, Prosthetic, Cosmetic and Periodontal interventions also. Thus, to establish a right treatment to this anomaly, the early proper examination and knowledge to recognize this anomaly is a prerequisite.
 | Figure 1. Intraoral Photograph showing co-joined 81 & 82
 |
 | Figure 2. IOPA Radiograph confirming presence of all permanent teeth
|
 | Figure 3. Intraoral Photograph showing Co-joined 82 & 83
|
 | Figure 4. IOPA Radiograph confirming partial anodontia with missing 42.
|
References
1. American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on oral health care/dental management of heritable dental development anomalies.Pediatr Dent. 2008-2009;30(suppl 7):196-201.
2. Terezhalmy GT, Riley CK. Gemination/fusion. Quintessences Int 1999:30:437
3. Neville BW, Damm DD, Allen CM, Bouquot JE, editors. Abnormalities of teeth. In: Oral and Maxillofacial Pathology. 2nd ed. W.B. Saunders Company; 2002. p. 75-77.
4. Ten Cate AR. Oral Histology: Development, Structure, and Function. St. Louis, MO: Mosby; 1998:81-102.
5. Krier PW. Complete fusion. Oral Surgery Oral Medicine Oral Pathology 1981; 52: 109.
6. Hitchin AD, Morris I. Geminated odontome: connation of the incisors in the dog, its etiology and ontogeny. Journal of Dental Research 1966; 45: 575–583.
7. Tannenbaum KA, Alling EE. Case reports of gemination and twinning. Oral Surgery 1963; 16: 883–887.
8. Guimarães Cabral LA, Firoozmand LM, Dias Almeida J. Double teeth in primary dentition: Report of two clinical cases. Med Oral Pathol Oral Cir Buccal 2008; 13 : E77-80.
9. Gellin ME. The distribution of anomalies of primary anterior teeth and their effect on the permanent successors. Dent Clin North Am. 1984;28:69-80.
10. Grahnen H., Granath, L.E. Numerical variations in the primary dentition and their correlation with the permanent dentition. Odontol Revy 12:348-57, 1961.
11. Clayton JM. Congenital dental anomalies occurring in 3,557 children. J Dent Child 23:206-8, 1956.
12. Neves AA., Neves ML., Farinhas JA. Bilateral connation of permanent mandibular incisors: a case report. Int J Pediatr Dent. 2002;12:61–5.
13. Schuurs AHB, Loveren C Van. Double teeth: Review of the literature. ASDC J Dent Child. 2000, Sept: 313-325.
14. Mader CL. Fusion of teeth. J Am Dent Assoc. 1979; 98:62–64
15. Alpoz AR, Munanoglu D,Oncag O. Mandibular bilateral fusion in primary dentition: Case report. J Dent Child(Chic), 2003;70:74-6.
|