|
|
|
| Modified Technique For Artificial Saliva Reservoirs In Maxillary Denture |
Varun Kumar 1 , Amrinder Singh Tuli 2 , Leena Tomar 3 , Babita 4 , Saraswati Rana 5 , Himanshu Shekhawat 6
1 Reader, Dept. Of Prosthodontics & Implantology - K.D Dental College, Mathura
2 Reader, Dept. Of Periodontics - Himachal Dental College, Sundernagar
3 Professor, Dept. Of Prosthodontics & Implantology - D.J.College Of Dental Sciences & Research, Modinagar
4 Assistant Professor Dept. Of Conservative Dentistry & Endodontics - Faculty Of Dentistry, Jamia Millia Islamia
5 PG Student, Dept. Of Prosthodontics - D.J.College Of Dental Sciences & Research, Modinagar
6 Senior Lecturer, Dept. Of Prosthodontics & Implantology - Kalka Dental College, Meerut
|
| Address For Correspondence |
Dr. Varun Kumar, (Reader)
Dept. Of Prosthodontics & Implantology,
K.D Dental College
Mathura,Uttar Pradesh, India.
Email : drvarun_smile@yahoo.co.In
Mobile : 09719041000 |
| Abstract |
| Xerostomia is a relatively common complaint that can make the wearing of complete dentures very uncomfortable for affected individuals. To help overcome this problem, a number of techniques have been proposed for incorporating reservoirs, containing salivary substitutes into dentures. These have had varying degrees of success. This article presents a case report of a patient suffering from Xerostomia who was successfully treated with a new form of reservoir denture |
|
| Keywords |
| Artificial, Saliva, Maxillary, Xerostomia |
|
| Full Text |
Introduction
Xerostomia is the dryness of mouth from lack of normal secretions. Patient suffering from Xerostomia not only has dry mouth but also difficulty in normal oral and oropharyngeal functions including eating, speaking and swallowing etc. It also makes wearing of dentures very uncomfortable for affected individuals. To help overcome this problem, number of techniques have been proposed for incorporating reservoirs containing salivary substitutes into dentures with varying degrees of success.Patients suffering from Xerostomia may complain of not only a dry mouth, but also of difficulty in functions including eating, speaking and swallowing. Extreme discomfort in wearing dentures is a common complaint.[1] Depending upon the cause, a variety of treatment options areavailable to the clinician. In medication induced Xerostomia - discussion with a patient’s general medical practitioner. In severe Xerostomic cases - Saliva substitutes or salivary stimulants, Soft denture liners can be given.[2],[3] In cases where all treatment modalities have proven unsuccessful, the incorporation into dentures of reservoirs containing saliva substitute, has been proposed.[4],[5],[6] This article presents a case of a patient suffering from Xerostomia who was successfully treated with a new form of reservoir in maxillary denture where other treatment modalities had failed. This modified new technique resulted in a denture that provided good lubrication of the oral tissues, was easily cleaned by the wearer and was produced from routine denture materials also.[7],[8],[9]
Case Report
An forty-five year old female was referred to the Department of Prosthodontics, kalka dental college, meerut with a complaint of dry mouth and difficulty while speaking, eating.Patient’s medical history indicated that she was on a number of medications for increased blood pressure, osteoarthritis, and non-insulin dependent diabetes mellitus. Patients past dental history revealed that she had many sets of maxillary and mandibular dentures made in recent years but was always unable to wear the denture due to constant irritation. Patient’s mouth was noted to be very dry with cracks at the corner of the mouth.After a number of unsuccessful adjustments to the existing dentures, it was decided to construct a new set of maxillary and mandibular dentures.since the patient was suffering from Xerostomia a decision was made to incorporate a salivary reservoir in the new dentures. During this process, the patient’s physician was also contacted and the medications were reduced to alter to try and reduce the hypo salivation.
Procedure
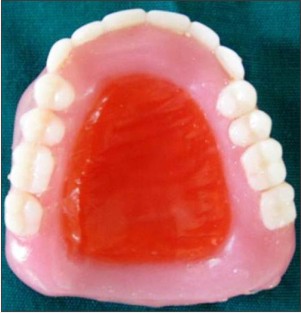
Clinically, primary and secondary impression wasmade in the normal manner. The maxilla-mandibular relationship was recorded with the mandible in retruded position and an acceptable freeway space. The models were then articulated in the normal way and the teeth set up for try in. After try in of the setup the reservoir was constructed. 2mm thick modelling wax was adapted over the entire palatal surface of the maxillary denture (Fig.1).The center of palatal wax wasthen removed. A rim of wax was left on the periphery to form the reservoir (Fig.2). The assembly was processed with heat cured acrylic resin (Fig.3). After the deflasking and polishing procedures were completed, wax was poured into the reservoir space (Fig.4). The separating medium was applied on the wax, another layer of wax was added on the previous layer and a lid was made(Fig.5). This second layer of wax was also processed with heat cure acrylic resin. This second layer of wax was also processed with heat cure acrylic resin (Fig.6, 7). Now the previous layer of wax was dewaxed and the lid was permanently attached to the denture with the help of autopolymerising acrylic resin(Fig.8). The completed assembly was smoothed and given a final polish. This allowed communication between the reservoir and the oral cavity. Then holes were made on the lid so as to facilitate communication between reservoir and the oral cavity (Fig.9). Drainage was tested by filling the reservoirs with water, placing the denture on a paper towel and checking that capillary action slowly drained the chambers.The patient was instructed about the filling of the reservoir and the due care. Post insertion checkup was done after a day and regular recall visits were scheduled. The patient was satisfied with the prosthesis.
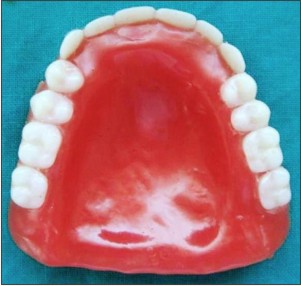 | Fig.1 : Adaptationofmodellingover the entire palatal surface of the maxillarydenture.
 |
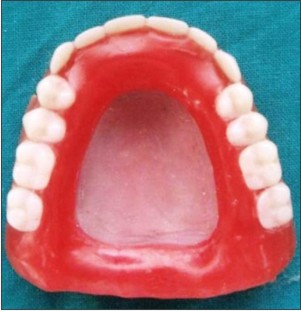 | Fig.2 : The center of palatal wax removed. A rim of wax was left on the periphery to form the reservoir.
|
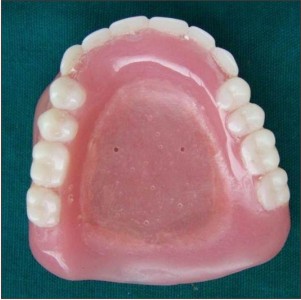
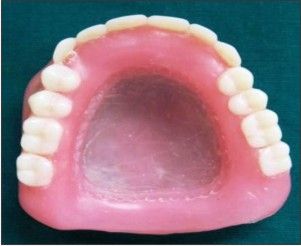 | Fig.3 : Finished and polished denture
|
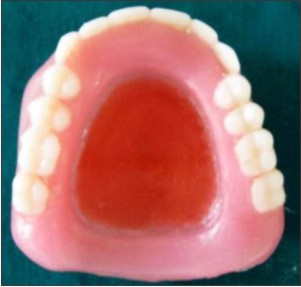 | Fig.4 : wax poured into the reservoir space
|
 | Fig.5 : Another layer of wax was added on the previous layer and a lid was made
|
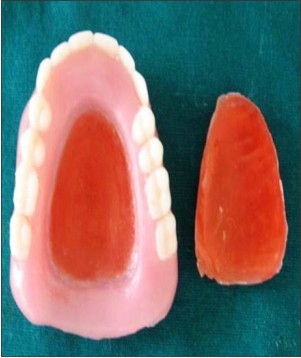 | Fig.6 : Wax lid separated from the denture
|
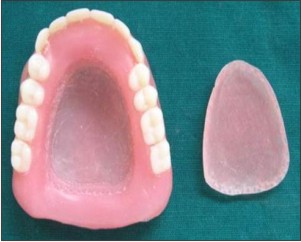 | Fig.7 : Lid processed with heat cure acrylic resin.
|
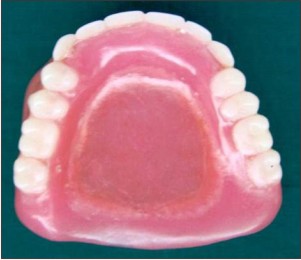 | Fig.8 : Final prosthesis
|
 | Fig.9 : Holes were made on the lid so as to facilitate communication between reservoir and the oral cavity
|
Discussion
Placement of reservoir in the maxillary dentures has been documented well in the literature. This technique in the maxillary denture offers clinicians an alternative method of treating patients suffering from Xerostomia. Advantage of this technique apart from lubrication of the oral tissues is that it also enables the patient to clearly visualize the levels of saliva substitute within the chamber. It allows easy cleaning and adjustment of the reservoirs as needed. The only drawback of the technique is the additional laboratory steps but it can be of great utility in cases of Xerostomia.Case selection is extremely important. Cutting reservoirs into the denture weakens its structure, so only cases with sufficient vertical dimension and thickness are suitable for this technique.From a clinician’s perspective, the clinical stages during construction are routine and require little additional chair-side time. Laboratory stages are time consuming and precision is essential to ensure accurate and smoothly fitting segments. Maxillary denture with artificial saliva reservoir resulted in a reservoir denture that provided good lubrication of the oral tissues was easily cleaned by the wearer and was produced from routine denture materials.Patient was instructed to flush out the reservoirs weekly with 1% per cent sodium hypochlorite solution. Orthodontic wire was provided to clean the drainage holes if they became blocked.The patient was also advised to continue to use the same salivary substitute as different brands varied in their viscosity and this would require alteration to the diameter of the drainage holes. After a number of follow up appointments, the patient was able to wear the denture comfortably throughout the day and only needed to refill the reservoirs twice per day.
Conclusion
This article reports a novel technique for the construction of a maxillary denture incorporating salivary reservoir. Xerostomic patients wearing prosthesis can benefit immensely from it. Incorporation of artificial saliva reservoir in the denture offers clinicians an alternative method of treating patients suffering from Xerostomia where other treatment modalities may have failed.
References
1. Al-Hashimi I. The management ofSjogren’s syndrome in dental practice. J Am Dent Assoc. 2001;132:1409–1417.
2. Stewart CM, Berg KM, et al. Salivary dysfunction and quality of life in Sjogren’s syndrome: a critical oral-systemic connection. J Am Dent Assoc. 2008;139:291–299.
3. Smith QT. Xerostomia and salivary substitutes. Northwest Dent. 1981;60:90.
4. Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134(1):61–69.
5. Sinclair GF, Frost PM, Walter JD. New design for an artificial saliva reservoir for the mandibular complete denture.J Prosthet Dent. 1996;75:276–280.
6. Mendosa AR, Tomlinson MJ. The split denture: a new technique for artificial saliva reservoirs in mandibular dentures. Aust Dent J. 2003;48:190–194.
7. Toljanic JA, Zucuskie TG. Use of a palatal reservoir in denture patients with Xerostomia.J Prosthet Dent. 1984;52:540–544.
8. Davis AN. A comparison of artificial saliva and chewing gum in the management of xerostomia in patients with advanced cancer. Palliat Med. 2000;14:197–203.
9. Hirvikangas M, Posh J, Makila E. Treatment of xerostomia through use of dentures containing reservoirs of saliva substitute. Proc Finn Dent Soc. 1989;85:47–50.
|
|
|
|
|
|
|