Introduction
Tooth surface loss is a frequent pathology encountered in elderly population. It is mulifactorial in origin including behavioral changes, unbalanced diet, various medical conditions and medications inducing acid regurgitation or influencing saliva composition and flow rate. The essence of management is an effective preventive regime; however, in severe tooth surface loss indirect complete restorations are necessary.[1]
Anterior guidance is crucial in human occlusion because it influences molar disclusion that controls horizontal forces. Loss of anterior guidance can result from severe wear of anterior teeth, which protects the posterior teeth during excursive movement. The collapse of posterior teeth results in the loss of normal occlusal plane and the reduction of the vertical dimension.[2],[3]. The molar disclusion is determined by the cusp-shape and the angle of hinge rotation[5],[6]. The twin stage technique developed by Hobo and Takayama reproduces disocclusion and anterior guidance more precisely and scientifically. It is based on the mathematical analyses of mandibular movement.[4]
During prosthetic treatment the condylar path has been used as the main determinant of occlusion. However in using the twin-stage procedure the cusp angle is used as the main determinant of occlusion which accurately controls the amount of disocclusion on the restorations without measuring the condylar path[7],[8],[9]. Embryologically, the cusp angle is an independent factor from both condylar and incisal paths. The objective of the present article is to describe the use of twin-stage technique to treat a severely worn out dentition with reduced vertical dimension of occlusion.
Case Report
A patient aged 60 years reported to the department of Prosthodontics, with the chief complaint of sharp teeth hurting his tongue while chewing. Patient’s medical history revelaed that he was suffering from gastroesophageal reflux disorder since ten years and was on medication for the same. Intra oral examination revealed generalized attrition and erosion with a loss of vertical dimension. There was 6 mm of freeway space present. The treatment plan included full mouth rehabilitation with complete coverage crowns to restore the lost vertical dimension of occlusion. The Hobo’s twin stage technique was chosen as it is based on mathematical analysis of mandibular movement giving importance for both disocclusion and anterior guidance, thus reducing the harmful horizontal occlusal forces and also it utilizes less chairside time.
Clinical Procedure:
Step 1 - Occlusal splint to raise the lost vertical dimension
An occlusal splint 3 mm in thickness was fabricated using heat cure acrylic resin to restore the lost vertical dimension, as there was 6 mm of freeway space (Fig 1). After the insertion of the splint the patient was examined on the first week and there after every two weeks for next two months. Meanwhile the patient was undergoing endodontic treatment for the required teeth.
Step 2 – Restoration of damaged teeth
The teeth which had undergone endontic treatment were restored to the normal clinical crown contours using appropriate core build-up materials.
Step 3 - Preparation of teeth to receive crowns
All the maxillary and mandibular teeth were prepared in a single visit to receive individual crowns on each tooth (Fig 2). Impressions were made and casts poured in dental stone to fabricate provisional restorations.
Step 4 – Facebow transfer
Facebow recording was done and transferred to the semi-adjustable articulator (Hanau wideview).
Step 5 - Centric relation record
The centric relation was recorded using a leaf gauge and the mounting of the casts to the articulator completed.
Step 6 - Provisionalization
Acrylic provisional crowns were provided with 3 mm increase in vertical dimension. The provisional restorations not only verify the increase in vertical dimension but also help to check the esthetic outcome of the treatment (Fig 3). The patient was followed for the next one month. After a satisfactory outcome with the provisionals the patient was posted for the permanent restorations.
Step 7 - Impressions for the final restoration
Provisional crowns were removed and impressions made for fabricating the permanent crowns. Impressions were made using additional silicone putty-reline technique and casts poured in Type IV die stone. Face bow transfer and centric relations re-recorded and casts mounted on to the articulator in the usual manner.
Step 8 – Hobo’s twin stage technique
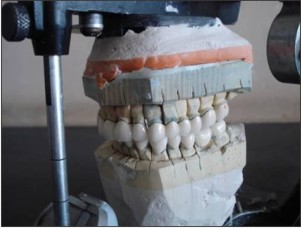
The anterior segment of the maxillary cast is removed for waxing up the posterior teeth (Fig 4). This prevents interferences from the anterior teeth. The articulator was adjusted for the condylar path and anterior guidance for condition 1 (Table 1). Wax-up for posterior was completed using Broadrick occlusal plane analyzer for establishing the occlusal plane.
Step 9 – Wax-up of anterior teeth
The articulator was adjusted for Condition 2 for waxing up the anterior teeth.
Step 10 - Try-in of ceramo-metal copings
The ceramo-metal copings were tried-in for both the maxillary and mandibular teeth.
Step 11 - Bisque try in
The ceramic build-up was done on the metal copings using the wax up as a guide to develop the tooth contours (Fig 6). The ceramic crowns were tried in the patient’s mouth.
Step 12 - Remounting and occlusal corrections
Occlusal corrections were carried out before final cementation by using a facebow transfer. The crowns were polished and glazed for the final cementation.
Step 13 - Anterior teeth cementation
First the maxillary and mandibular anterior teeth were cemented and protrusive interferences are removed (Fig 7).
Step 14 - Posterior teeth cementation
Next the posterior teeth were cemented and post insertion instructions given.
Step 15 - Post operative recall
The patient was instructed for regular recall visits for the next one month. A soft splint was fabricated to prevent damage to the restorations (Fig 8) as he was found suffering from nocturnal bruxism.
 | Figure 1: Occlusal Splint 3 Mm In Thickness To Raise The Lost Vertical Dimension Of Occlusion
 |
 | Figure 2: Preparation Of Teeth To Receive Individual Crowns On Each Tooth
|
 | Figure 3: Acrylic Provisionals In Place To Check The Esthetic Outcome Of The Treatment
|
 | Figure 4: The Anterior Segment Of The Maxillary Cast Is Removed For Waxing Up The Posterior Teeth
|
 | Figure 5: Try-in Of Ceramo-metal Copings
|
 | Figure 6: The Completed Ceramic Restorations In The Articulator
|
 | Figure 7: Anterior Teeth Cementation
|
 | Figure 8: A Soft Splint In Place To Prevent Damage To The Restorations
|
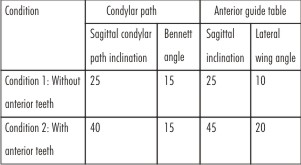 | Table 1: Articulator adjustment values for the twin-stage procedure (deg.)
|
Discussion
Full mouth rehabilitation is challenging and often involves complicated clinical and laboratory procedures. The success of treatment depends on diagnostic skills, perceptual treatment planning and by using more appropriate technique for rehabilitation. A critical aspect in treating such patients is to determine the occlusal vertical dimension and adopt a systematic approach that can lead to a proper predictable and favorable treatment prognosis[11],[12]. There has been a conflicting opinion on whether to work simultaneously or work on different segments of the arch individually. Full-mouth reconstructions involving full arch preparations, impressions, provisional restorations, and master casts are regarded as simultaneous reconstructions. Various techniques may be used in simultaneous constructions to obtain complete arch dies and mounted casts. These techniques assist in concomitant laboratory construction of the units. When all of the prepared teeth are on a single articulator, there is flexibility in developing the occlusal plane, occlusal theme, embrasures, crown contour and esthetics. But the disadvantages include arduous, unpredictable patient visits, full arch anesthesia, full arch chairside treatment restorations, multiple occlusal records, and possible loss of the vertical dimension of occlusion[13],[14],[15]. Full-mouth rehabilitation can be done by completing one quadrant before beginning with the other. The advantages of such an approach are that it is primarily chairside and includes preparation and final impressions of select teeth, maintenance of vertical dimension, quadrant anesthesia, and shorter appointments. The disadvantages include restrictions for achieving ideal occlusion when altering the vertical dimension, occlusal plane and embrasure development.
The twin stage technique developed by Hobo and Takayama which reproduces disocclusion and anterior guidance more precisely and scientifically. It differs from the existing techniques of occlusal reconstruction and is based on scientific data and mathematical analyses of mandibular movement. In using the twin-stage procedure the cusp angle is used as the main determinant of occlusion which accurately controls the amount of disocclusion on the restorations without measuring the condylar path. The average calibrations of condylar, lateral and incisal guidance and cusp angle provide an easy approach of management with lesser skills needed.
Conclusion:
Rehabilitation of a mutilated dentition should focus not only on the functional and esthetics aspect of the dentition but also improve upon the health of the whole stomatognathic system. A detailed diagnosis and treatment planning is necessary to achieve predictable success in such cases. Full mouth rehabilitation using Hobo’s twin stage technique is an easy, less time consuming and accurate method of rehabilitation which can be conveniently adopted to provide predictable results.
References:
1. Dietschi D and Argente AA. comprehensive and conservative approach for the restoration of abrasion and erosion. Part II: clinical procedures and case report. Eur J Esthet Dent. 2011; 6: 142-159.
2. Kar AK, Parkash H and Jain V. Full-mouth rehabilitation of a case of generalized enamel hypoplasia using a twin-stage procedure. Contemp Clin Dent. 2010; 1: 98-102.
3. Banerjee S, Chakraborty N, Singh R and Gupta T. Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure. Contemp Clin Dent. 2012; 3: 103-7.
4. Hobo S and Takayama H. Twin-stage procedure. Part 1: A new method to reproduce precise eccentric occlusal relations. Int J Periodontics Restorative Dent. 1997; 17: 112-123.
5. Agrawal M, Sankeshwari B, Pattanshetti CV. Use of zirconia to restore severely worn dentition: a case report. Case Rep Dent. 2012: 324597. Epub 2012 Sep 5.
6. Moslehifard E, Nikzad S, Geraminpanah F, Mahboub F. Full-mouth rehabilitation of a patient with severely worn dentition and uneven occlusal plane: a clinical report. J Prosthodont. 2012; 21(1): 56-64.
7. Hausman M, Hobo S. Occlusal reconstruction using transitional crowns. J Prosthet Dent. 1961; 11: 278–287.
8. Braly BV. A preliminary wax-up as a diagnostic aid in occlusal rehabilitation. J Prosthet Dent. 1966; 16: 728–730.
9. Kazis H. Complete mouth rehabilitation through restoration of lost vertical dimension. J Am Dent Assoc. 1948; 37: 19–39.
|