Introduction
Oligodontia is defined as a condition characterized by congenital absence of six or more teeth excluding the third molars. The anomaly can occur as an isolated disorder or as a part of a syndrome. These two forms are referred to as oligodontia/I (isolated oligodontia) and oligodontia/S (oligodontia as part of a syndrome). Patients with oligodontia/S may have abnormalities of skin, ears, eyes and bones in association with the dental symptoms. The disorder has been reported to be associated with Ectodermal dysplasia, Rieger syndrome, Ectrodactyly-Ectodermal dysplasia- Clefting syndrome, Bloch-Sulzberger syndrome, and Cutis marmorata teleangiectatica congental.[1]
The causes of missing teeth may be broadly classified into general which encompasses all those cases where the cause is genetic and local factors that include early irradiation of tooth germs, hormonal and metabolic influences, trauma and osteomyelitis. Congenital absence of teeth can be a consequence of physical obstruction or disruption of dental lamina, space limitation, functional abnormalities of the dental epithelium and failure of initiation of the underlying mesenchyme.[2]
Oligodontia is a disorder, which any pedodontist can come across in his daily practice. So, early diagnosis is essential for the development of treatment strategies that are needed to manage the continuum of continued growth and development along with varying aesthetic and functional needs of the patient until growth is complete and definitive restorations can be placed.
Case Report
A 9-year-old girl reported to the department of Pedodontics and Preventive Dentistry, Government Dental College, Rohtak for decayed teeth. The patient was in good health and her medical history was non-contributory. Intraoral examination of the patient revealed multiple missing teeth. The following teeth were present:
54, 53, 52, 51, 61, 62, 63, 64
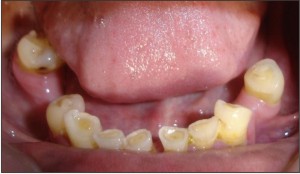
85, 83, 82, 81, 71, 72, 73, 75
Both the primary maxillary first molars were cariously involved. The primary maxillary second molars were missing.
Family history revealed multiple missing teeth in the father also. Intraoral examination of the girl’s father revealed that following teeth were present
15, 13, 12, 11, 21, 23, 28
48, 44, 43, 42, 41, 31, 32, 33, 35
Radiographic finding
Radiographic examination of the patient was done using intraoral periapical radiographs and orthopantomograph. Orthopantomogram revealed that
18, 17, 16, 15, 25, 26, 27, 28
48, 47, 46, 45, 41, 31, 35, 36, 37, 38
were missing.
Radiographic examination of the patient’s father showed that
18, 17, 16, 14, 22, 24, 25, 26, 27
47, 46, 45, 34, 36, 37, 38
were missing with the history of extraction of 18, 27, 38.
Treatment
Pulp therapy was performed in the cariously involved teeth and permanent restorations placed. Removable acrylic partial dentures were fabricated to improve the masticatory efficiency. Modification of the existing dentures will be done as the patient grows and permanent teeth erupt.
 | Fig. 1 Intraoral photograph of maxillary arch of the patient
 |
 | Fig. 2 Intraoral photograph of mandibular arch of the patient
|
 | Fig. 3 Orthopantamograph of the patient
|
 | Fig. 4 Intraoral photograph of maxillary arch of the father
|
 | Fig. 5 Intraoral photograph of mandibular arch of the father
|
 | Fig. 6 Orthopantamograph of the father
|
 | Fig. 7 Removable partial denture inserted in maxillary arch
|
Discussion
The prevalence rate for missing teeth has been reported to be 0.1-0.9% in the primary dentition and 3.5-6.5% in the permanent dentition.[3] Assuming third molars to be the most frequently missing teeth, the next most frequently missing teeth are mandibular second premolars (2.8%), maxillary lateral incisors (1.6%), maxillary second premolars and mandibular incisors (0.23-0.8%).[4],[5] In the primary dentition maxillary lateral incisors are twice as likely to be missing as mandibular lateral incisors. Congenital absence of the remaining primary teeth is rare. However, strong relationship has been shown between missing primary teeth and permanent successors by Daugaard-Jensen et al; who showed that hypodontia in the primary dentition was always associated with hypodontia of the permanent dentition.[6]
Balit reported that not all teeth are equally heritable. The “key” tooth in each morphologic class has the highest heritability, and is the more stable tooth morphologically. The more distal a tooth, for example, lateral incisors and second premolars, the more it seems to be influenced by environment. Maxillary central incisors and maxillary and mandibular first molars have been shown to be the most stable teeth.[7] Hypodontia affecting teeth that are rarely missing for example first permanent molars was usually associated with missing primary teeth.[1] In the present case both the permanent maxillary first were missing which is a very rare finding.
A genetic component of oligodontia has also been suggested. Erpenstein and Pfeiffer described X-linked inheritance of oligodontia or hypodontia through four generations of a family.[9] A mutation in the MSX1 and PAX9 gene has been reported to be associated with the disorder.[9],[10]
It is known that from around 9 years of age, children with disabilities realize that they are different from other children. This realization may in turn produce depression in the child. So, the dental team plays a vital role in helping the young child to cope with the issues of attractiveness during the formative years.
The role of pediatric dentist includes
Behavior management of the disabled child,
Prevention of caries in the remaining dentition,
Maintenance of oral hygiene,
Restoration of function by intermediate restoration of diminutive teeth and placement of dentures.
Management of spacing and maloccluded teeth by orthodontic treatment[2]
Restorative problems encountered in patients with multiple missing teeth reflect the quality of available alveolar bone and occlusal disturbance. Absence of teeth causes a significant deficit in the alveolar bone height and quality. Another problem that one comes across is eruption of permanent teeth into poor positions and supraeruption of unopposed posterior teeth. The overall effect is a deep overbite, reduced interocclusal space and lower facial height.
Such patients need to be looked after by multidisciplinary teams. Close liaison between the surgeon, orthodontist and pediatric dentist is crucial to maximize the outcome.
References
1 Weide YS, Steen WHA, Bosman FA. Distribution of missing teeth and tooth morphology in patients with oligodontia. J Dent Child 1992; 59: 133-140
2 Nunn JH, Cater NE, Gillgrass TJ, Hobson RS, Jepson NJ, Meechen JG et al. The interdisciplinary management of hypodontia: background and role of pediatric dentistry. Br Dent J 2003; 194: 245-251
3 Brook AH. Dental anomalies of number, form and size: their prevalence in British school children. J Int Assoc Dent Child 1974; 5: 37-53
4 Grahnen H. Hypodontia in the permanent dentition. Clinical and genetic investigations. Thesis. Odont Revy 1956; 7(Suppl): 3
5 Cameron J, Sanpsom WJ. Hypodontia of permanent dentition. Case reports. Aust Dent J 1996; 41: 1-5
6 Daugaard-Jensen J, Nodal m, Skovgaard LT, Kjaer I. Comparison of the pattern of agenesis in the primary and permanent dentitions in a population characterized by agenesis in the primary dentition. Int J Paed Dent 1997(b); 7: 143-148
7 Balit HL. Dental variations among populations, an anthropologic view. Dent Clin N Am 1975; 19: 125-139
8 Erpensein H, Pfeiffer RA. Geschlechsgebunden- dominant erbliche zahnunter zahl. Human genetic 1967; 4: 280-293
9 Vastardis H, Karimbux N, Guthua SW, Seidman JG, Seidman CE. A human MSX1 homeodomain missence mutation causes selective tooth agenesis. Nature Genetics 1996; 13:417-421
10 Stockton DW et al: Mutation of PAX9 in association with oligodontia. Nature Genetics 2000; 24: 18-19
|