Introduction
With advancement in dentine adhesives and the evolution of esthetic dentistry, composites have become more widely used as posterior restorations. In choosing posterior composite materials, a clinician may consider their mechanical properties, handling properties and marginal sealing ability. Proper handling and use of adequate technique should ideally lead to a restoration with perfect wall adaptation that is free of porosities and voids.
Most studies consider the presence of voids and porosities as disadvantage for the restorations. Voids at the margin of the restoration may lead to gross microleakage and discoloration. Second, the initial stress concentration around the voids will result in a lower resistance to fatigue and increased wear[1],[2],[3]. Third, voids between successive increments in a composite will have a negative effect on the flexure strength of the material. Fourth, voids can appear as translucent area on radiographs and may be misinterpreted as secondary caries.[4] To overcome all the demerits of voids and porosities, various techniques and materials have been tried by dentist.
In this study we have used recently developed innovative technique i.e. ‘snow plough technique’ along with future packable composite i.e. (ormocer). In this technique, a layer of flowable composite (i.e. 0.5-1mm) was injected over the pulpal floor, axial wall and gingival seat and left uncured. Subsequently, a second layer of composite with higher viscosity was applied into the cavity. This resulted in the flowable composite being extruded from the cavity by the more viscous material. After removing the excess material, the restoration was cured for 40 seconds from occlusal surface.
This in vitro study is another effort to reduce number of voids and porosities in CL-II resin composites by using different techniques and different composites.
Materials and Methods
This study was undertaken in the Department of Conservative Dentistry and Endodontics, Bapuji Dental College and Hospital, Davangere, using following materials and method.
Materials:
1. Acid etchant ( Scotchbond multipurpose, 3M)
2. Boding agent (Single bond, 3M)
3. Packable composite (Admira, voco)
4. Acid etchant (Admira, voco)
5. Bonding agent (Admira,voco)
6. Hybrid composite (Z-100,3M)
7. Flowable composite ( Filtek, 3M)
 |
 |
 |
|
 |
|
 |
|
 |
|
Equipments:
1. Visible light cure unit with radiometer (Confident ,India)
2. Stereomicroscope (Leica wildM3Z, Germany)
Methods:
Forty eight freshly extracted human molars were collected, scaled and stored in normal saline. Standardized CL-II cavities were prepared with straight fissure diamond point of diameter 0.8mm (Horico, Japan) in a high speed turbine. Cavities were approximately 2mm in width bucco-lingually, 3mm deep occluso gingivally. The margins were located 1 to 1.5mm above the cementoenamel junction.
All the cavities were etched for 15 seconds with 34% phosphoric acid, washed for 10 seconds and excess water was very briefly blown away, leaving a moist surface. The cavities were then covered with an adhesive agent and cured for 20 seconds with a light curing unit (Confident,India) having light intensity of 450mW/cm2 (radiometer). A steel matrix (Hanenkratt, Germany) was applied with a tofflemeir retainer (Hanenkratt, Germany). The cavities were restored using different composites of different viscosities employing different insertion technique (i.e. Layering and snowplough). Restorations were finished and polished with super snap kit (Shofu,Japan). Forty eight teeth were randomly divided into six groups
 |
|
 |
|
 |
|
 |
|
 |
|
Group I: (Flowable lining and hybrid / snowplough):
Cavities were lined with flowable composite to about 0.5mm occlusogingival thickness followed by 2mm increment of hybrid composite i.e. Z-100 (medium viscous) to expel flowable composite. Curing was done for 40 seconds. Remaining cavity was incremently filled with Z-100.
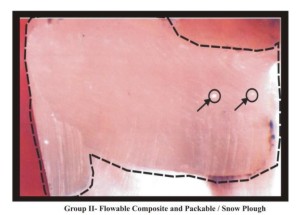
Group II: (Flowable lining and packable/snowplough):
Cavity preparations were restored with same protocol as given in group-1 but instead of hybrid composite (medium viscous), packable composite (highly viscous) was used.
Group III: (Flowable liner (precured) / hybrid composite):
Cavity preparations were lined with thin layer of flowable composite (i.e. 0.5 to 1mm) and cured for 20 seconds. Remaining cavity was filled with hybrid composite(medium viscous) in increments and each increment cured for 40 seconds.
Group IV: (Flowable liner (pre cured)\packable composite):
Cavity preparations were restored with same protocol as in group-3 but instead of hybrid composite, packable composite( highly viscous) was used.
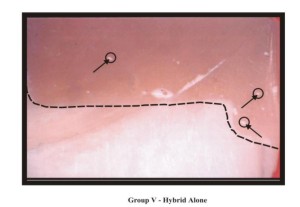
Group V (Hybrid alone):
Cavity preparations were filled in increments with hybrid composite (i.e. medium viscous) and each increment cured for 40 seconds.
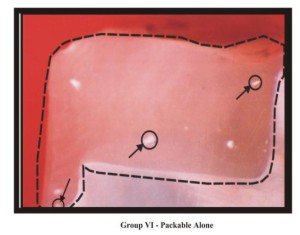
Group VI (packable alone):
Cavity preparations were filled in increment with packable composite (i.e. highly viscous) and each increment cured for 4 seconds.
Restorations were stored for 24 hours and then sectioned through the middle of restoration in a mesio-distal direction along their long axis with a diamond disc (0.5mm) and observed under 50X stereomicroscope.
Voids were seen in three sites: Occlusal half, Cervical half & Gingival interface
Voids were scored as follows
0 = No voids
1 = Voids present
Statistical Analysis
Fisher’s exact test was used to determine whether significant differences were present between two groups. A p value of 0.05 or less was considered as statistically significant. P < 0.05 significant, p > 0.05 Nonsignificant
Results:
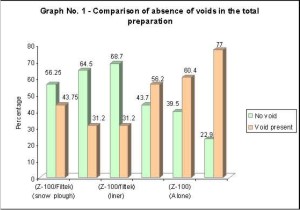
Graph-I summarizes the result of absence of voids inside the restoration. Total voids were evaluated by combining the three sites of the internal voids. Group–III [z-100\ filtek(precured)] showed minimum number of voids. Results for total number of voids absent can be expressed in following order i.e. III > II > I > IV > V > VI.
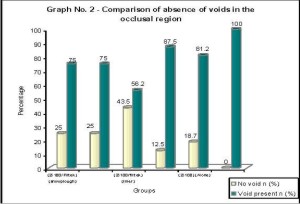
Graph-II lists the absence of occlusal voids. Group–III showed least number of voids. Resuts for absence of voids in occlusal part can be expressed in following order III>I>II>IV>V>VI.
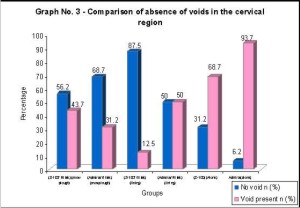
Graph-III lists absence of voids at cervical region. Least number of voids were seen in group III .Results for cervical part can be represented in following order III > II > I > IV > V > VI. Thus use of flowable composite lining clearly reduced likelihood of cervical voids.
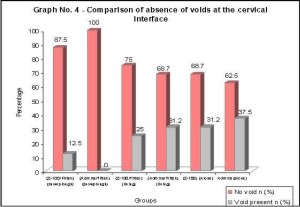
Graph-IV lists the absence of gingival interface voids. Least number of interface voids can be seen in group II. Group II showed all the restorations free of voids.Result for gingival interface voids can
Discussion
Introduction of composites was a major break through in the field of esthetic dentistry. Composite which forms a bonafide part of esthetic dental treatment, remains technique sensitive and abounds with lot of controversies
One of most important controversial topic related to composite is voids. The porosity of dental composite resins has been identified as a factor that may adversely affect critical properties of the final restoration, such as diametral tensile strength, abrasion resistance water sorption, degree of cure, surface roughness and colour stability etc.[4],[5],[6],[7]
In general, porosity creates bulk or surface geometrical discontinuities, which increases fracture propagation and failure probability on loading.[3],[8],[9]
Flowable composite were developed in 1996. Flowable composite also exhibited a lower modulus of elasticity to resist polymerization shrinkage due their increased stress buffering capacity. The low modulus materials employed as cavity liners may reduce contraction stress at the tooth restoration interface.[59]
Packable composite were introduced in 1996 having filler size 0.8 m and 82% by wt. These materials are simply stiffer and less sticky than traditional composites, which allow them to be packed more easily.[30]
Restoring CL-II cavities with composite resin has always remained point of debate. This study is yet another effort to solve the overwhelming problem of voids concerning CL-II composite restorations. In the present study, this new ‘SnowploughTechnique’ was used along with recently introduced packable composite i.e. ormocer to evaluate the voids.
The results showed that groups with flowable composites as a liner had lesser number of voids. Groups (III, II, I, IV) had lesser voids in total preparation as compared to group (V and VI).
Voids in total preparation:
On comparison of total number of voids in restorations in group- I (Z-100 / Filtek) using. snowplough technique showed 56.25% of restoration sites free of voids and group II (Admira/Filtek) using snowplough technique showed 64.5% restoration sites free of voids. This was because of this technique which maintains minimal volume of flowable composite to increase cavity adaptation and reduce potential from marginal gap formation. Comparison of group-I and group-II shows non significant difference.[33]
Group III (Z-100/Filtek) where filtek was precured showed 68.7% of restoration sites free of voids i.e. highest percent among all the groups due to presence of flowable composite as a liner which leads to better adaptation and act as a stress breaker. Flowable composite possess more stress-buffering capacity due to low modulus of elasticity, hence it resists polymerization shrinkage [59]
Occlusal Region:
When occlusal area was viewed for the voids, group-1 showed only four restorations free of voids. Similar results were obtained for group-II. Most of studies using snowplough technique showed decrease in number of occlusal voids in CL-II restoration[10]. But in present study, voids were seen in occlusal area. It suggested improper compaction of various increments of composite resin. Furthermore, it is possible that porosities were already present inside the composite material61. Group-III showed maximum number of restorations (I.E. 7) 43.5% free of occlusal voids due to better adaptation of thin and medium consistency composites as compared to thick consistency composites along adjacent increment.
Cervical Region
When cervical area was screened for voids, results for group-I (56.2%) and group-II (43.7%) showed most of restorations free of voids with snowplough technique which was not as good as group –III (87.5%) in which liner was cured first. These results are similar to study conducted by Chung S.F et al (2004).10 Group-III in which liner was cured showed minimum number of voids as flowable liner which has low modulus of elasticity acts as stress breaker to reduce contraction stresses on the tooth restoration interface.
Gingival Interface:
At the gingival interface, results showed group-I (87.5%) and group II (100%) of restorations free of voids. In group II (100%), all restorations were completely free of voids at gingival interface due to snowplough technique which was utilized in this group. This technique maintains a minimal volume of flowable composite to increase cavity adaptation and reduces the potential for marginal gap formation33. Similar results were seen in recent study conducted by S.F. Chung et al.[10]
Group-III (75%) and group-IV (68.7%) where flowable composite used as a liner (procured) also showed more number of restorations free of voids at gingival interface due to better adaptability of flowable composite and also acts as stress breaker to reduce polymerization shrinkage stresses.[59] These results were similar to many studies done previously.[9],[10]
In this study, the use of flowable composite lining significantly reduced the incidence of voids. Group I and group II in which snowplough technique was used, voids were considerably reduced at gingival interface which is a critical part of Cl-II cavities. Based on the results of this study, the technique is recommended as simple and practically applicable to Cl-II resin restorations.
Conclusion:
Based on the results of this study, the technique (i.e. snow plough or modified incremental technique) is recommended as simple and practically applicable to Cl-II resin restorations.
References:
1. O’Brien WJ, Yee J. Microstructure of posterior restoration of resin composite after clinical wear. Operative Dentistry 1980; 5: 90-94.
2. Leinfelder KF, Roberson TM. Clinical evaluation of posterior composite resins. Gen Dent 1983; 31: 276-280
3. McCabe JF, Ogden AR. The relationship between porosity, compressive fatigue limit and wear in the resin composite restorative materials. Dental Material 1987; 3: 9-12.
4. Jan WV Van Dijken, Eystein Ruyter I, Roy I Holland. Porosity in posterior composite resins. Scand J Dent Res 1986; 94: 471-8.
5. DeGee AJ. Some aspects of vacuum mixing of composite resin and its effect on porosity. Quintessence Int. 10th report, 1978: 1778.
6. Jorgenson KD. Restorative resin abrasion Vs mechanical properties. Scandinavian Jol of Dental Research 1980; 88: 557.
7. Voleke CF and Duggar TOD. The porosity and roughness of four direct filling resin. Jol of Oral Rehabilitation 1981; 8: 507.
8. Asmussen EK and Jorgensen KD. Fatigue strength of some resinous material. Scandinavian Jol of Dental Research 1982; 92: 257-261.
9. Leinfelder KF, Mclartha CD and Wisniewki JF. Posterior composite a critical review. Jol Ala Dent Assoc 1981; 69: 19-25.
10. Kerjci I, Lutz F, Krejci D. The influence of different base materials on marginal adaptation and wear on conventional Cl-II composite restoration. Qiuintessence Int 1988; 19: 191-198. |