Introduction
Although research suggest the causes of dry socket are not fully understood ,it also suggest that the bacterial contamination is a major etiological factor, attempt to prevent its occurrence have this focused on reducing oral microbes within the wound either through oral administration of antibiotics or local application of antiseptic solution.
Dry socket was first described by Crawford in 1896.Several other terms have been used in referring to this condition have been used such as Alveolar osteitis, Localized osteitis, Post operative Alveolitis , Alveolalgia, Alveolitis sicca dolorosa, Septic socket, Necrotic socket, Localized Osteomyelitis, fibrinolytic osteomyelitis.
Dry socket following the extraction of mandibular third molar is an important post operative problem for both patient and surgeon.
Dr. Kurt Thoma stated that “Alveolar osteitis is a condition in which blood clot disintegrates; at first the clot has dirty grey appearance and then it falls out, leaving a bony socket bare of granulation tissue, suppuration is absent, but foul odor is present and severe neuralgic pain persists for days”. The symptoms generally set in on second or third day after the extraction of tooth, and last for 10 to 40 days.
Birn labeled the complication “Fibrinolytic aveolitis”, which is probably the most accurate of all the terms. Fibrinolysis with subsequent loss of blood clot is believed to the general cause of alveolar osteitis .As the primary role of bacteria in this process has been documented ,the most effective method for reducing dry socket has been through the use of agents that systemically or topically reduce oral microbes in wound.several risk factors have been identified in association with dry socket,these include excessive use of elevators and difficulty in extraction, an inexperienced surgeon, tobacco or oral contraceptive use, the use of pre operative steroids ,the use of local anesthetic with vasoconstrictor and inadequate irrigation during and after the extraction.
Because rinsing with chlorhexidine has been shown to reduce the quantity of oral microbe populations and this may be effective in reducing the incidence of dry socket.
The purpose of this study is to determine the effectiveness of chlorhexidine solution used as preoperative and post operative rinse in reduction of dry socket after third molar extraction.
Material and Methods
This study was conducted on100 patients in age group 15 to 60 years were selected on the basis of requirement of removal of mandibular third molar. Only those patients who were healthy and free from any medical complications were selected.
The patients were divided in two groups,
Group 1- patients for this study received no special pre and post operative oral hygiene procedure.
Group 2- patients received 15ml of chlorhexidine rinse for 30 seconds before the procedure and irrigation of the extracted socket was done with chlorhexidine and patients were asked to rinse the mouth with 15ml chlorhexidine for 30 seconds twice daily for one week after 24 hours of extraction.
Extraction Of Mandibular Third Molar:
Procedure: after all the pre-operative investigation were carried out, the patients were taken up for extraction. Patient were made to sit comfortably in dental chair.
Anesthesia: this was obtained through the inferior alveolar nerve block, lingual nerve block; long buccal nerve block .2% lignocaine hydrochloride with 1:80,000 adrenalines was used as an anesthetic agent.
Removal Of Tooth: The third molar tooth which were covered with soft tissue were exposed by giving relieving incision with B.P handle no. 3 and blade no.15 .After retraction of gingiva the tooth was delivered from the socket by elevator and forceps.
In Group 1 patients no special oral hygiene measures were used and in Group 2 patients, their mouth was irrigated with 15ml of chlorhexidine before procedure and tooth socket was irrigated with chlorhexidine.
Wound Closure: Wound was closed with 3-0 black silk sutures. After the wound was closed with sutures, the gauze pack was kept for 30 minutes and the patients were advised to follow pos-operative instructions.
Follow Up: patients were recalled after 7 days for check up and suture removal or sooner if pain persisted. On return visits, extraction sockets were evaluated for abnormal healing, presence of necrotic tissue and absence of clot.
Dry socket was developed 72 hours after surgery resenting as persistent pain, absence of clot, fetid smell. Patients who had not returned before one week were questioned about increase in pain during post-operative period in their subsequent visits.
 | Instruments
 |
 | Administration of local anaesthesia
|
 | Suturing
|
 | Relieving incision
|
 | Healing after 7 days of extraction without chlorhexidine rinses
|
 | Socket after extraction
|
 | Healing after 7 days of extraction with chlorhexidine
|
 | Healing of extraction without chlorhexidine rinse
|
 | Healing of extracted socket with chlorhexidine rinses
|
Stastical Analysis
Categorical data are expressed as percentages and comparison was done either by Chi-square test or Fisher’s Exact Test. Mean duration of surgery between two groups was compared by Student’s test. A P-value of less than 0.05 was considered for statistical significance.
Results
Results of this study showed that there are significant differences between the both groups .In Group 1 patient there was increased incidence of dry socket compared to Group 2 patients.
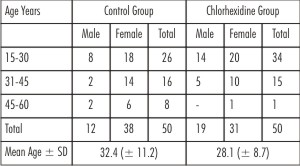
Age and Sex wise distribution: (Table 1) Patients were ranged from 15 to 60 years. Out of 100 patients 69 patients were female and 31 male. They were categorized into different age groups 15-30, 31-45, 45-60 years.
 | Table - 1 : Age and Sex Wise Distributio
|
In Group 1, 38 female patients and 12 male patients and in Group 2, 31 female and 19 male patients were there. Total 10 patients developed dry socket, 7 patients are female.
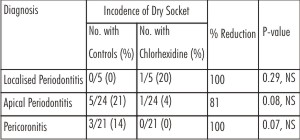
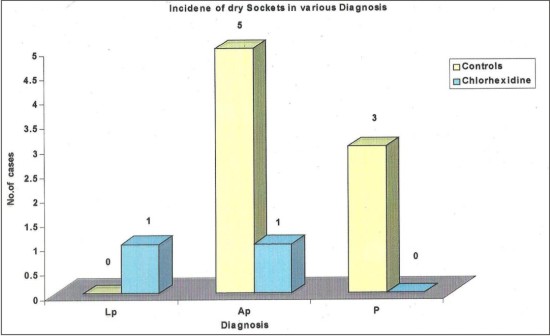
Incidence of Dry Socket in Relation to Diagnosis: (Table 2): Patients were categorized according to diagnosis i.e. localized periodontitis, apical periodontitis and Pericoronitis. 10 patients were diagnosed having localized periodontitis, were divided into two groups consisting of 5 patients each, one patient developed dry socket in group 2. Patients those diagnosed under apical periodontitis total 6 patients developed dry socket. In Group 1, 5/24 (21%) and in Group 2, 1/24 (4%) developed dry socket. There was 81% reduction in incidence of dry socket compared to Group 1. Patient with Pericoronitis in Group 1, 3/21 (14%) and in Group 2, 0/21 (0%) developed dry socket .there was 100% reduction in the incidence of dry socket. Although reduction rate of dry socket was high but the results are not significant.
 | Table - II Incidence of Dry Socket in Relation To Diagnosis
|
 | Table - III : Incidence of Dry Socket in Relation to Various Factors Under Study
|
 | Table - IV : Incidence of Dry Socket in Control and Chlorhexidine Groups (3-7 Days)
|
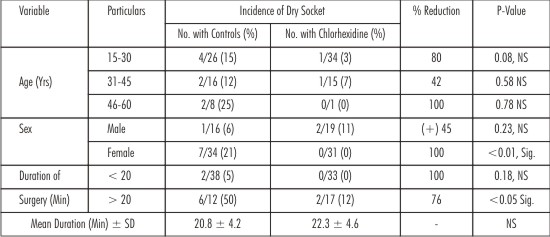
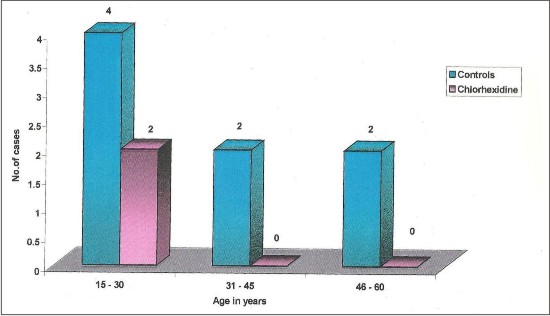
Incidence of Dry Socket in relation to various Factors under Study (Table 3): Here the patients were categorized according to Age/Sex and duration of surgery. Incidence of dry socket was higher in age 45-60 years 2/8 (25%). Chlorhexidine showed effectiveness in reduction of incidence of dry socket irrespective of age.
In sex wise distribution out of 7/69 female patients developed dry socket and in chlorhexidine group no female patient developed dry socket the result are statistically significant(P<0.01).
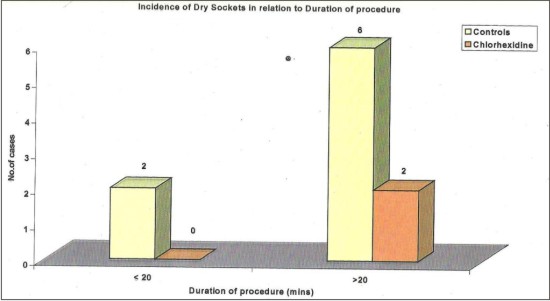
According to duration of surgery as the time of surgery increases the incidence of dry socket is more. Chlorhexidine showed 76% reduction in the incidence of dry socket compared with Group 1.Results are statistically significant (P<0.05).
Incidence of Dry Socket in Group1 and Group 2 patients (Table 4):
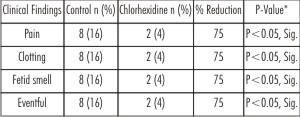
In overall incidence of dry socket 8/50 (16%) patients developed dry socket in Group 1.In Group 2, 2/50 (4%) patient developed dry socket. There is overall 75% reduction in the incidence of dry socket compared to Group 1 and results are statistically significant (P<0.05).
 | Graph 1
|
 | Graph 2
|
 | Graph 3
|
So results of this study showed that there is significant decrease in incidence of dry socket when compared to patient who received no special oral hygiene procedure and results also showed that as the duration of surgery increases, in older age group and in female patients’ incidence of dry socket is more. Chlorhexidine rinses also show reduction in incidence of dry socket in these patients.
Discussion
The results of this study demonstrate that the pre and post-operative use of chlorhexidine is an effective preventative measure of dry socket after extraction of mandibular third molars. In comparison with control group, dry socket rate in chlorhexidine group was reduced by 75%(0.05%).these findings are consistent with what has been reported in existing literature, which taken collectively suggests that chlorhexidine reduces extraction site-level dry socket rates by 25% to 80% after the extraction of mandibular third molars. (Table 5).
The rinsing regimens varied across these studies and included pre operative or post operative rinsing alone, pre operative and post operative rinsing together, at the time of surgery, which may in part explain the variation in dry socket reductions observed in the studies. However, the consistency of a treatment effect across the study suggests that variations in rinsing regimens, with respect to whether rinsing was pre operative, post operative or both, were less significant than the length and mechanism of delivery (rinse versus irrigation) of the dosing regimen. Rinsing regimens less than 7 days in duration show less reduction in dry sockets. Even in two studies by (Berwick and Lessin and Tjernberg) that failed to demonstrate a statistically difference between chlorhexidine and control therapy ; substantial reduction in the incidence of dry socket of 24.5 % and 80.2 % respectively, were reported in the chlorhexidine group as compared with the placebo group.
Chlorhexidine Perioperative rinse therapy has consistently been shown to deliver a substantial reduction in the incidence of dry socket after surgery. In contrast with the use of chlorhexidine, Perioperative use of the anti microbial rinse povidone-iodine has been reported to be generally ineffective as a preventive for dry socket (Sweet J.B).
Local antibiotic therapies involving tetracycline and Clindamycin have also been reported to be effective in preventive dry socket (Swanson).
Evidence suggesting that bacterial contamination is a major etiological factor has been demonstrated repeatedly. An increase incidence of dry socket occurs in the presence of periapical infection, Pericoronitis, gingivitis, periodontitis and in patients with poor oral hygiene. (Awang M.N.).
Patients with high perioperative and post operative oral microbial counts have a higher incidence of dry socket (Brown L.R.).
Oral rinses with 0.2% chlorhexidine is active against both aerobic and anaerobic, gram negative and gram positive organisms as well as yeast. It has high affinity for cell wall of microorganism and induces changes in the surface structure, resulting in the loss of osmotic equilibrium and precipitation of the cytoplasm. In addition to immediate killing of bacteria during rinsing, chlorhexidine binds to anionic surfaces of the oral cavity and then gradually released to provide a continuing bacteriostatic effect. Rinsing and irrigation with chlorhexidine preoperatively and during surgery is likely to reduce bacterial contamination of the surgical site.
Reduction in the incidence of dry socket can be achieved with the use of a chlorhexidine solution as an immediate pre-surgical rinse, irrigation of the extracted socket, and a 7 days post-operative home rinse programme.
Although an attempt is made to evaluate the incidence of dry socket. It was not possible to achieve statistically significant results when data broken down into sub groups may be more number of cases needed for each sub group to set significant result. It should not be overlooked that, overall incidence of dry socket is reduced up to 75% when compared with control group and results are statistically significant (0.05%).
Summary and Conclusion:
1) Total 100 patients were evaluated for present study.
2) They were divided in to two groups- without rinse and with chlorhexidine rinse.
3) Both male and female patients were selected for study.
4) In female patients there are more chances of formation of dry socket.
5) As the duration of procedure increases the incidence of dry socket is more.
6) Dry socket is more prevalent in higher age group.
7) Patient who used chlorhexidine mouth rinses showed reduction in number of dry sockets as compared to patients who used no special oral hygiene measures.
8) Chlorhexidine oral rinses are effective measures in prevention of dry socket, and wound healing.
References
1. Awang M. N: The etiology of dry socket: A review. Int. Dent. J. 1989; 39; 236-40.
2. Berwick M.J.E. and Lessin ME. : Effects of a chlorhexidine gluconate oral rinse on incidence of alveolar osteitis in mandibular third molar surgery. J Oral Maxillofac Surg. 1990; 48: 444-448.
3. Bonine F.L.: Effect of chlorhexidine rinse on the incidence of dry socket in impacted mandibular third molar extraction sites. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79: 154-158.
4. Brown L.R., Merrill S.S. et al: Microbiology study of intra oral wounds. J Oral Surg. 1970; 28: 89-95.
5. Hermesch C.B., Hilton T.J., Biesbrock A.R. et al: Perioperative use of 0.12% chlorhexidine gluconate for the prevention of alveolar osteitis. Oral Surg Oral Med Oral Pathol Oral Radiol endod. 1998; 85: 381-387.
6. Keith G Smith: Chlorhexidine gel reduces incidence of alveolar osteitis after extraction of the mandibular third molars. Evid Based Dent. 2009; 10 (2) 54-55.
7. Larsen P.E: The effect of a chlorhexidine rinse on the incidence of alveolar osteitis following the surgical removal of impacted mandibular third molars. J Oral Maxillofac Surg. 1991; 49: 932-937.
8. M.P Minguez-Serra, C Salort-Liorca and F-J Silvestre-Donat: Chlorhexidine in prevention of dry socket: effectiveness of different dosage forms and regimens. Med Oral Patol Oral Cir Buccal 2009 Sep. 14 (9): e445-9.
9. Penarrocha M., Sanchis J.M., Saez U. et al: Oral hygiene and post operative pain after mandibular third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92: 260-264.
10. Pilar Hita-Iglesias, Daniel Torres-Lagares. Et al: Effectiveness of chlorhexidine gel versus chlorhexidine rinse in reducing alveolar osteitis in mandibular third molar surgery. J Oral Maxillofac Surg 2008 Mar: 66 (3) 441-445.
11. Rango J.R and Szkutnik A.J.: Evaluation of 0.12% chlorhexidine rinse on prevention of alveolar osteitis. Oral Surg Oral Med Oral Pathol. 1991; 72: 524-526.
12. Swanson A.E. : Prevention of dry socket: An overview. Oral Surg Oral Med Oral Pathol. 1990; 70: 131-136.
13. Sweet J.B and Macynski A.A.: Effect of antimicrobial mouth rinses on the incidence of localized alveolitis and infection following mandibular third molar surgery. Oral Surg Oral Med Oral Pathol. 1985; 59: 24-26.
14. Tjernberg Arne: Influence of oral hygiene measures on the development of alveolitis sicca dolorosa after surgical removal of mandibular third molars. Int J Oral Surg. 1979; 8: 430-434. |