Introduction
The term abrasion is used to indicate the wear that occurs on a tooth from the friction of a foreign body. Abrasion is the mechanical wearing away of tooth substance by abnormal mechanical process.[1], [2], [3]. It is a non carious cervical lesion, marked by the loss of dental hard tissue in the cervical part of the tooth, not caused by caries, multicausal and insufficiently clarified etiology. It has been estimated that twenty five percent of tooth destruction does not originate from caries process commonly widespread problems are tooth wear. Tooth wear is a pathological wear to supplementary to dental caries. Among tooth wear the preventable and self- inflicted is abrasion.[4],[5],[6],[7],[8]
Abrasion of hard dental tissue is an escalating predicament, reflects changing life style and social pressure. Numerous studies reported that abrasion is a multifactorial process. [9],[10],[11],[12],[13]. Widespread causes documented as positive agents for abrasion are aggressive, horizontal tooth brushing and use of abrasive dentifrices and other indigenous abrasive agents especially used by Indian population. The degree of wear depends on the orientation of brushing, force and frequency applied for cleaning and abrasive effect of material used for cleaning.[14],[15],[16],[17],[18] The literature shows a wide range of prevalence of abrasion ranging from 5% to 85%. This wide range in results is a consequence of the different methodologies and diagnostic criteria. Prevalence increases with age and lesions are seen more frequently in males than in females. [6], [9], [14], [19],[20],[21],[22]
In the current study it was intended to quantify the prevalence of abrasive lesions of teeth in the residents of Bhopal City of Central India. Literature on prevalence of abrasion of teeth is scarce and the public health significance is largely indefinite. Not much information is yet available on incidence and reported prevalence among Indian population. Abrasion of teeth is to a certain limit self- inflicted, which can be prevented to an immense extent with appropriate instruction and impetus. The present study attempts to provide a basis of estimating abrasion of teeth in a population and its etiological factors. This may contribute for development of national or regional oral health program, planning appropriate health education strategies to suggest possible remedial measures.
Materials and Methods
A survey was conducted in Bhopal city of Central India to assess the abrasive lesions of teeth. The present study is based on 598 persons aged 18 to 59 and above; 307 being women and 291 men. The cross- sectional study relates the prevalence of abrasive lesions and is association of etiological factors. Epidemiological parameters are considered in the light of individual tooth brushing technique and tooth brushing frequency and also of the stiffness of the tooth brush and the abrasivity of the dentifrices
General information in sequence regarding dietary habits and medical history were collected by questionnaire. Examination of abrasion recorded with the help of tooth wear index Smith and Knight (modified)[23]. The investigator conducted the survey single-handedly and prior to the start of the survey training and calibration was carried out. After training and retraining final concordance to determine the diagnostic variability agreement for assessment was 94%. During the survey at the end of the day 10 subjects were re-examined to maintain intra-examiner consistency. Considering the prevalence rate of abrasion to be 50% with the type 1 error of 5% and the power of the study to be 90%, the sample size was calculated to be 500 adults.
As per information from Bhopal City Corporation and ensured randomness and representativeness total 598 available subjects were examined. The study focused into the assortment of age groups from 18 to 59 years. The sampling universe was the entire city of Bhopal.
Tooth brushing technique was judged on the basis of individuals own demonstrations of the brushing habit as horizontal, vertical and circular. Brushing frequency measured as once a day, twice a day or more than twice a day. Stiffness of the bristles is measured according to the manufacturer as Soft, medium and hard. Clearly identifiable wedge shaped lesions present on the cervical areas were recorded as abrasion in the present study. Enamel losses on other surfaces like incisal, palatal, interproximal etc. surfaces have been excluded. Individuals having minimal 20 teeth were included in the study. Exclusion criteria included was teeth with ortho treatment and crown -bridges.
Statistical Method included cross tabulations and regression analysis. SPSS package 17 version was used. Regression analysis was done to evaluate the risk factors where a dependent variable (abrasion) in relation to series of independent variables to know the cause and effect in the prevalence of abrasion was done. Chi-square test was applied. P value less than 0.05 was considered statistically significant.
Results:
The data collected among residents of Bhopal city of Central India was analyzed and the results showed the following:
A total of 598 subjects were examined in age groups of 18-59 years and above of both sexes out of which291 males and 307 females respectively. [Table 1]
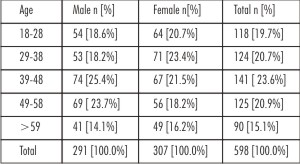 | Table 1: Demographic Profile Of The Study Population Of Bhopal City According To Age And Sex.
 |
The overall prevalence of abrasion was 68.6% [Table 1]. The abrasive lesions although multifactorial increased with age. In the present study abrasive lesions are in ascending order with age and the difference between youngest age group and all other age groups are statistically significant. Abrasive lesion of teeth does not show any sex predilection [Table 2].
The results of the regression model are summarized: [Table 3]
 | Table 2 :Prevalence of abrasion according to age among the residents of Bhopal city.
|
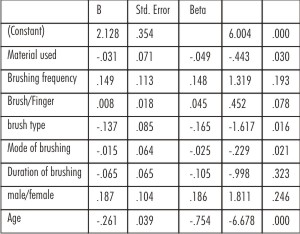 | Table 3: Variables having a cause and effect relation with abrasion (regression model).
|
The number of lesions recorded varied as a consequence of the brushing habit used. Lesions predominated in the horizontal mode of brushing and were least frequent in the individuals with circular technique. This holds true both among people who brush their teeth with indigenous material and those using finger predominantly in place of brush.
It is evident all that in all age groups lesions are more frequent among those who use horizontal brushing and abrasive materials to clean their teeth. The difference is statistically significant for those who use toothpaste paste and soft bristle tooth brush.
Abrasive Lesions does not show any difference statistically with increasing frequency of cleaning and the duration of brushing.
Discussion
The etiology of cervical abrasion is multifactorial and consistent. It has been clear that reprehensible tooth brushing and if coarse materials used for oral hygiene upkeep plays an important influence in instigating abrasion.[24],[25] The present results confirms akin on the population level, an association between improper tooth brushing, coarse materials used to clean teeth and abrasion.[26],[27] The overall occurrence of abrasion was found to be 68.6% among residents of Bhopal District. This is in favor with the Croatian study[28] where tooth wear is 60-70% and the prevalence and severity of tooth abrasion appeared to increase with age this finding is also supported by two other studies among adult population in Turkey and the Southeast of England respectively.[29], [30] The prevalence observed in the study by Smith & Robb in the European population accounts 25-60% [29] which a broader perspective where with the age there is advancement of abrasion, present study shows analogous finding. Another study reported 10-35% of enamel cervical wear among adolescents in South London by Bartlett et al[31] Which appeared very low so not in agreement with this study as the adolescents were the target group. Sagnes and Gjermo1976 reported similarly high levels of enamel wear in cervical lesion. This pattern was different from Nigerian experience[32] where prevalence is 15.8%. There is a probable linking between oral hygiene practices and abrasion. This is different from that observed in European countries[29] combination of abrasive erosive lesion is pragmatic could be related with contemporary life style habits and diet. On contrary 35.8% abrasion stated in the study of tooth wear patterns and their associated etiologies in adults in Kelantan, Malaysia.[33]
Bergstorn and Lavestd reported the prevalence of abrasion 31% amid the residence of Stockholm. [34] Present study reveals a huge chunk of abrasion among the residents of Bhopal District.
Fairly more extent of prevalence could be attributed to wide spread ignorance and lack of knowledge. Residents of Bhopal City were using cheap and low grade materials for oral hygiene maintenance hence more amid rural populations. Other explanation could be due to cultural believes and slow transition. This attributed to established lack of awareness regarding oral hygiene practices with abrasive wear, multifactorial process concluded by most of the studies similar findings are reflected in this study too.[34], [35], [36], [37]
Cervical wear is a common condition.
The distribution of the subjects according to gender does not show any discernible divergence and is statistically insignificant. Current study also shows abrasion is evenly disseminated between both the sexes. Bergstron J and Lavstedt, Randentz, Barnet and Cutright also reported no statistical dissimilarity owing to gender.[34], [37],[38]
In the present investigation the concept of tooth brushing was separated to consist of five independent variable brushing technique, brushing frequency, bristle stiffness and abrasivity of the material used and duration of brushing. Of these five variables the correlation of abrasion was stronger with brushing technique and use of abrasives as dentifrice. Where as influence by bristle stiffness and frequency of brushing and duration of brushing was weak. However age of the individuals exhibited the strongest correlation to abrasion. In this connection age may be the expression, with increase in chronicity of tooth brushing and the use of abrasives for cleaning the teeth increases proportionately so is the abrasive lesion. The present study exhibits similar findings. The individuals with horizontal brushing for a longer and use of abrasives as oral hygiene aid reveals higher level of abrasion. The present study is in concordance with this expectancy as the probability of cervical abrasion increases with increase in age with other studies.[31],[32],[33],[34],[36],[38]
Together, age and brushing frequency expression for accumulated brushing time in the individuals. The importance of accumulated brushing time for the development of abrasive lesions is indicated that only subjects with least abrasion are youngest age group could be less exposure to abrasive cleaning aids and harmful brushing technique.[34],[36],[38]
Horizontal brushing strokes invariably causes abrasion, in vivo it is proved that faulty tooth brushing has a significant role in causing abrasion. In the present result confirms this expectancy and shows horizontal brushing is most hazardous and likely to produce abrasion than any other technique. Circular or vertical tooth brushing strokes are the safest for causing the pathological wear in the form of abrasion.
Most studies pertaining to the abrasion potential of the material used for cleaning teeth agree that the abrasives incorporated do cause damage. The present study reflects the parallel conclusion. Coarser the material higher will be the abrasive lesions. The use of more indigenous material are much harmful and causes more amount of abrasiveness in teeth accumulated affect is visible in later decades of life.[31],[32],[34]
Limitations of the study
Factors of possible importance to dental abrasion which were omitted in the study are the pressure of the tooth brush applied and indirect etiologies like acidic oral environment and easy enamel dissolution and medication. Some of he biological factors such as saliva, tooth composition and structure, occlusion and behavioral factors were not considered. Further investigations and continuous follow up may allow the mapping of the relationship of biological factors with the occurrence of tooth wear.
Conclusion
The progression rate of abrasion is not constant, since the progression by time is not linear. The increasing order is proportionate to the age. To conclude from previous and present literature on abrasion, ample evidence exist a relationship between tooth brushing action, abrasive use to clean teeth and manifestation of abrasion. Individual oriented factors especially tooth brushing technique, duration of brushing and frequency of brushing exerts greater influence in formation of abrasion. Individuals are furnished with appropriate prophylactic measures that are effective for oral cleanliness but still harmless to oral tissues.
Improper tooth brushing and rampant use of abrasives to clean teeth, reprehensible brushing habits and lack of becoming accustomed to superlative habits of hygiene among populations are the add on in the prevalence of abrasion.Abrasion of hard dental tissue is an escalating predicament, reflects changing life style and social pressure. Numerous studies reported that abrasion is a multifactorial process. Most common cause is use of abrasive dentifrices coupled with injudicious use of horizontal tooth brushing pattern.
Abrasion being a self inflicted destructive process the damage and mortality due to this can be preventable by effective health instruction and inspiration. In order to prevent this problem from becoming worse and become a burden. We should try to combat the problem from its early stages. Literacy and wakefulness are important steps in achieving superior oral health of people. Masses are encouraged to discontinue the habit of using abrasives and to use the tooth paste and brush and become accustomed to a correct method and proper oral hygiene measures. Government should supply these products on subsidized rates. Audiovisual aids like television might promote the accurate aid and acceptable process to maintain oral hygiene.
References:
1. Bjorn, H; &Lindhe, J: Abrasion of dentine by tooth brush and dentrifice. Odontol. Revy 1966:17:17-27
2. Frostell,G.&Lindstrom,G: Undersokningaravnagraav den svenskamarknadenstandkramer. Del I. odontol.ForrenTidskr. 1964: 29: 211-248
3. Miller, W.D.: Experiments and observation on the wasting of tooth tissue. Dent.Cosmos 1907: 49:109 -116.
4. Marzouk; 1997: Operative Dentistry- “ Modern theory and practice” 418-420.
5. Eccles JD 1982 Tooth surface loss from abrasion, attrition and erosion. Den Update 9: 373-374, 380-381
6. EffaratHabsha in 1999. “The etiology and pathogenesis of tooth wear.’ Oral Health.” 1999, 83-91
7. Mair L H 1992. Wear in Dentistry – Current terminology. J. Dent 20: 140-144
8. Pindborg JJ 2007 Pathology of the dental hard tissues. Is ted Copenhagen, Munksgaard.
9. SognnaesRF,Wolcott RB, Xhonga FA 1972, Dental erosion I. Erosion like patterns occurring in association with other dental conditions. J.Amer Dent Assoc 84:571-576
10. Brady and Wood RD 1977. Scanning microscopy of cervical erosion J. Am. Dent.Assoc. 94:726-729.
11. Lee WC and Eakle WS, 1984. Possible role of tensile stress in the etiology of cervical lesion of maxillary premolar- a finite element investigation. J. Prosthet Dent 52:374-380.
12. Manly RS, Wiren J, Manly PJ, Keene RC 1965 Amethod for measurement of abrasion of dentine by tooth brush and dentrifrice. J. dent Res. 44: 533-540
13. Osborne-Smith, E.J.T. Burke and N.H.F. Wilson in 1999. “The etiology of non carious cervical lesions. Int. Dent Jnl 1999: 49; 139-143.
14. Volpe AR Mooney R, ZimbrunnenC,Stahl D, Golman HN 1975. “A long term clinical study evaluating the effect of dentrifrices in oral tissues.” J.Perio46: 113-118
15. Mannerberg 1960.“Appearance of tooth surface as observed in shadowed replicas in various age group in long term studies after brushing in case of erosion and after exposure to citrus fruits.” Odontol Rehab 11 supp 70-86.
16. Krames, P: The prevalence of tooth root exposure and the relation of the extent of such exposure to the degree of abrasion in different age classes. J.Dent.Res 1941:20:565-581.
17. Sangnes,G&Gjermo,P: Prevalence of oral soft and hard tissue lesions related to mechanical toothcleansingprocedures.Community Dent. Oral Epidem. 1976:4:77-83.
18. Epstein.S&Tainter,M.L: Abrasion of teeth by commercial dentrifices. J.Amer.Dent.Assoc 1943:30:1036-1045.
19. Anneruth,G.&Poppeiman,A. Histological evaluation of gingival damage by tooth brushing. An experimental study in dog. ActaOdontolScand 1975:33:119-127.
20. Gilson.M; Charbeneau G &Hill.C: A comparison of physical properties of several soft tooth brushes. J. Mich.Dent.Assoc 1969:51:347-361
21. Teaford and Tylender et al; 1991: “ a new approach to the study of tooth wear.” IntnJnl Of Den Res: 70(30) : 204-207
22. Bishop K et al; May 1997. “Wear now? An update on the etiology of tooth wear.” Quintessence Int: 28(25): 305-13.
23. Smith BG,Knight JK 1984. An index for measuring the wear of teeth. Dent J 1984; 156:435-8
24. Smith BG,Knight JK A comparison of pattern of tooth wear with etiological factors. Br.Dent. Jour 157:16-19
25. Radentz WH,Barmes GP, Cutright DE 1976. “A survey of factors associated with cervical abrasions of tooth surface. J. Perio. 47: 148-154
26. Jan Bergerstrom and StigLavenstedt 1979. An epidemiologic approach to tooth brushing and dental abrasion. Commu dent. Oral Epidemiol 1979: 7:57-64
27. Spranger H 1995. Investigation into the genesis of angular lesions at the cervical lesion of teeth Review] Quintessence Intern 26:149-154.
28. Borcic J, Anic, Urek MM, Ferreri S 2004 . The prevalence of non-carious cervical lesions in permanent dentition. J. Oral Rehabilitation 31:117-123.
29. Smith BG and Robb ND 1996. Prevalence of tooth wear in 1007 dental patients. J.OralRehabil 23:232:239.
30. Akgul HM, Akgul N, Kaoglanoglu S, Ozdabak N 2003. A survey of the corresepondence between abrasion and tooth brushing habits in Erzurum. Turkey. Intn Dent. J 53: 491-495
31. Bartlett DW, Coward PY, NikkahC,Wilson RF (1998). The prevalence of tooth wear in a cluster sample of adolescent school children and its relationship with potential explanatory factors. Br.Dent J 184:125-129.
32. OginniAO,andOlusile AO, Udoye CL (2003) Non-carious cervical lesion in a Nigerian population: Abrasion or abfraction? Int Dent J 49: 139-143.
33. Wirdatul R Daly, Wan ZaripahwanBakar, Adam Husien, NoorlizaMasrtura, Ismail, Bennet T and Amaechi (2010).The study of tooth wear patterns and their associated aetiologies in adults in Kelantan, Malaysia. Archives of Orofacial Sciences 5(2):47-52
34. Bergstrom J, Lavestdt S 1979: “ An epidemiological approach to tooth brushing and dental abrasion.” Comm. Dent. Oral Epidem. 7: 57-64
35. Tomasik M (2006) . Analysis of Etiological factors involved in non carious cervical lesions. Ann Acad Med Stetin 52 (3):125-136.
36. Osborne-Smith, E.J.T. Burke and N.H.F. Wilson in 1999. “The etiology of non carious cervical lesions. Int. Dent Jnl 1999: 49; 139-143.
37. Radentz WH,Barmes GP, Cutright DE 1976. “A survey of factors associated with cervical abrasions of tooth surface. J. Perio. 47: 148-154
|