INTRODUCTION
Gingival recession, often called as tooth root exposure, is the denudation of the tooth root surface due to apical movement of gingiva1. As a result, there is wearing away of cementum, thereby exposing the underlying dentinal surface to the oral environment. Dentin exposure can also occur as a result of erosion, abrasion, attrition, hypoplastic enamel, defective restorations, improperly developed cementoenamel junction, caries, cracked tooth syndrome, trauma etc. Consequently, tooth hypersensitivity develops, which is described clinically as an exaggerated response to a non noxious sensory stimulus2. According to Wycoff, dental hypersensitivity is a painful response of a tooth to irritants such as tooth brushing, sweet and sour foods and thermal changes. It is a potential threat to individual’s oral health because such pain may interfere with maintainence of good oral hygiene3.
A variety of treatment modalities have been tried to overcome hypersensitivity with variable
success4 such as burnishing of exposed root surface to form a smear layer, topical application of agents that form insoluble precipitates, impregnation of tubules with plastic resins and application of dentine bonding agents to seal off the tubules. One such treatment procedure is to use desensitizing agents alongwith electric current so as to achieve deeper penetration5 and better results – the phenomenon known as Iontophoresis6,7,8. Iontophoresis deposits more of active ions into tooth substance and also the depth of penetration of the active ions is far greater than when topical application is given alone9. This might lead to a more lasting and predictable treatment of dentinal hypersensitivity.
In recent past, surgical procedures like coronally displaced flap, has also been
employed for the management of gingival recession10. It is a plastic and reconstructive surgical approach aimed at the restoration of the lost gingiva. Alongwith improving functional and hygienic aspects of the teeth and surrounding structures, it is also aimed at the improvement of cosmetic aspect as well11.
The purpose of this study was to compare the efficacy of a single iontophoretic application of 1% sodium fluoride with a combined approach of iontophoresis with 1% sodium fluoride and the coronal repositioning of the flap on the exposed root surfaces of the teeth, in the management of dentinal hypersensitivity.
MATERIALS AND METHOD
The study was conducted on the patients selected from the Outpatient Department of Punjab Government Dental College and Hospital, Amritsar. A total of twenty patients between 30 to 60 years of age, complaining of hypersensitivity on exposed root surfaces and recession not exceeding 3mm on both sides of the arch were selected. Chronic smokers and alcoholics, subjects taking anti-coagulant therapy and/or anti-inflammatory drugs or using desensitizing pastes or mouthwashes, subjects with chipped or cracked teeth, cervical caries, teeth with metallic restorations, inaccessible involved area, shallow vestibular depth, inadequate zone of attached gingiva and presence of any systemic disorder were not included in this study.
The teeth included in the study were divided into two groups: Group A (Teeth in the right quadrant) which received an iontophoretic application of 1% sodium fluoride solution at 1 mA current for 1 minute and Group B (Teeth in the left quadrant) which received the similar iontophoretic application but combined with a coronally repositioned flap operation.
Each group was further divided into two subgroups depending upon the type of stimuli used to grade the hypersensitivity. Subgroup a included subjects which received air blast stimulus and Subgroup b included subjects which received cold water stimulus.
This way the study was divided into four categories, each category included, one group and one subgroup viz.
1) Category I: Group A subgroup a
2) Category II: Group A subgroup b
3) Category III: Group B subgroup a
4) Category IV: Group B subgroup b
DIAGNOSTIC-CUM-EVALUATION TESTS
The teeth selected were rated for the degree of hypersensitivity according to a numerical verbal rating scale using air blast and cold water tests. In both tests, the patient was asked to rate the discomfort according to Verbal rating scale (from 0 to 4) and the same were recorded. The score concludes as 0=no discomfort, 1=mild discomfort, 2=moderate discomfort, 3=severe pain only during application and 4=severe pain persisting after removal of stimulus
IONTOPHORETIC UNIT
An apparatus was designed and fabricated for delivering a measurable amount of direct current for iontophoresis. It consisted of a 9 volt battery that supplied direct current of 9 volts, an ammeter with graduations ranging from 0 to 3 mA at differences of 0.05 mA each, a voltmeter from 0 to 10 volts, a variable resistance, a polarity selection switch, an on/off switch, an inactive electrode and an active electrode having a head of no. 7 camel hair brush for agent’s application.
1% SODIUM FLUORIDE SOLUTION
Commercially available sodium fluoride salt was weighed and stored in moisture resistant packings, weighing 100 mg each. At the time of application, fresh solution was prepared by dissolving one package of salt in 10 ml of distilled water.
METHOD
Group A: In group A, after phase I therapy, the selected teeth were dried and isolated with cotton rolls. The inactive electrode was held firmly, but lightly in contact with attached gingiva of the tooth receiving the application. The brush of the active electrode of the iontophoretic unit was dipped into 1% freshly prepared sodium fluoride solution, and applied on the exposed surface of the tooth. The current was switched on and the resistance knob was slowly turned clockwise till the reading was 1 mA. The brush was kept at the tooth surface for one minute without any movement so as to avoid its displacement to the adjacent gingiva.
Group B: In group B, after local anesthesia administration, the sulcular incision was given and a full thickness periodontal flap was raised. Entire surgical site was thoroughly debrided and irrigated profusely with 1% betadiene followed by normal saline solution. After that, a similar iontophoretic application of 1% sodium fluoride as given on the right side (Group A), at the same therapeutic dosage was applied. A semilunar incision was given in the alveolar mucosa of the concerned tooth and flap was repositioned coronally and interrupted sutures with 4-0 black silk thread were placed in each interdental space at the surgical site. Standard post-operative protocol was implemented.
improvement of cosmetic aspect as well11.
The purpose of this study was to compare the efficacy of a single iontophoretic application of 1% sodium fluoride with a combined approach of iontophoresis with 1% sodium fluoride and the coronal repositioning of the flap on the exposed root surfaces of the teeth, in the management of dentinal hypersensitivity.
MATERIALS AND METHOD
The study was conducted on the patients selected from the Outpatient Department of Punjab Government Dental College and Hospital, Amritsar. A total of twenty patients between 30 to 60 years of age, complaining of hypersensitivity on exposed root surfaces and recession not exceeding 3mm on both sides of the arch were selected. Chronic smokers and alcoholics, subjects taking anti-coagulant therapy and/or anti-inflammatory drugs or using desensitizing pastes or mouthwashes, subjects with chipped or cracked teeth, cervical caries, teeth with metallic restorations, inaccessible involved area, shallow vestibular depth, inadequate zone of attached gingiva and presence of any systemic disorder were not included in this study.
The teeth included in the study were divided into two groups: Group A (Teeth in the right quadrant) which received an iontophoretic application of 1% sodium fluoride solution at 1 mA current for 1 minute and Group B (Teeth in the left quadrant) which received the similar iontophoretic application but combined with a coronally repositioned flap operation.
Each group was further divided into two subgroups depending upon the type of stimuli used to grade the hypersensitivity. Subgroup a included subjects which received air blast stimulus and Subgroup b included subjects which received cold water stimulus.
This way the study was divided into four categories, each category included, one group and one subgroup viz.
1) Category I: Group A subgroup a
2) Category II: Group A subgroup b
3) Category III: Group B subgroup a
4) Category IV: Group B subgroup b
DIAGNOSTIC-CUM-EVALUATION TESTS
The teeth selected were rated for the degree of hypersensitivity according to a numerical verbal rating scale using air blast and cold water tests. In both tests, the patient was asked to rate the discomfort according to Verbal rating scale (from 0 to 4) and the same were recorded. The score concludes as 0=no discomfort, 1=mild discomfort, 2=moderate discomfort, 3=severe pain only during application and 4=severe pain persisting after removal of stimulus
IONTOPHORETIC UNIT
An apparatus was designed and fabricated for delivering a measurable amount of direct current for iontophoresis. It consisted of a 9 volt battery that supplied direct current of 9
volts, an ammeter with graduations ranging from 0 to 3 mA at differences of 0.05 mA each, a voltmeter from 0 to 10 volts, a variable resistance, a polarity selection switch, an on/off switch, an inactive electrode and an active electrode having a head of no. 7 camel hair brush for agent’s application.
1% SODIUM FLUORIDE SOLUTION
Commercially available sodium fluoride salt was weighed and stored in moisture resistant packings, weighing 100 mg each. At the time of application, fresh solution was prepared by dissolving one package of salt in 10 ml of distilled water.
METHOD
Group A: In group A, after phase I therapy, the selected teeth were dried and isolated with cotton rolls. The inactive electrode was held firmly, but lightly in contact with attached gingiva of the tooth receiving the application. The brush of the active electrode of the iontophoretic unit was dipped into 1% freshly prepared sodium fluoride solution, and applied on the exposed surface of the tooth. The current was switched on and the resistance knob was slowly turned clockwise till the reading was 1 mA. The brush was kept at the tooth surface for one minute without any movement so as to avoid its displacement to the adjacent gingiva.
Group B: In group B, after local anesthesia administration, the sulcular incision was given and a full thickness periodontal flap was raised. Entire surgical site was thoroughly debrided and irrigated profusely with 1% betadiene followed by normal saline solution. After that, a similar iontophoretic application of 1% sodium fluoride as given on the right side (Group A), at the same therapeutic dosage was applied. A semilunar incision was given in the alveolar mucosa of the concerned tooth and flap was repositioned coronally and interrupted sutures with 4-0 black silk thread were placed in each interdental space at the surgical site. Standard post-operative protocol was implemented.
RESULTS
The teeth were subjected to evaluation criteria after one, two, four, eight and twelve week’s period of observation. The hypersensitivity was recorded at each recall. Results thus obtained were put to statistical analysis.
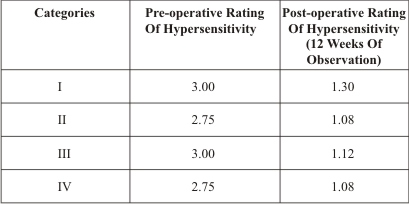
Table 1 (graph 1) shows the grand mean reduction in dentinal hypersensitivity in all four categories after 12 weeks of observation against the baseline level (i.e. preoperative mean dentinal hypersensitivity). In category I, the grand mean reduction was 1.30 over an observation period of 12 weeks against the baseline level of 3.00. Similarly, in category II, the grand mean reduction was 1.08 over an observation period of 12 weeks against the baseline level of 2.75. In category III, the grand mean reduction was 1.12 over an observation period of 12 weeks against the baseline level of 3.00. In category IV, the grand mean reduction was 1.08 over an observation period of 12 weeks against the baseline level of 2.75.
TABLE 1 :
Grand Mean Reduction in all categories after 12 weeks of observation against the baseline values
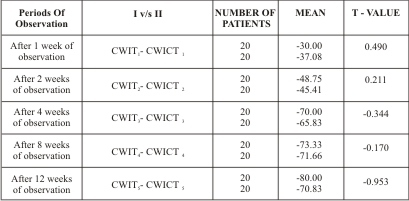
Table 2 & 3 (graph 2 & 3) shows that there was a significant reduction in dentinal hypersensitivity, irrespective of the stimuli used, by both iontophoretic application alone and similar iontophoretic application combined with coronally repositioned flap.
TABLE 2 :
showing comparison of the reduction in mean percentage change in dentinal hypersensitivity at different periods of observation in category I and II
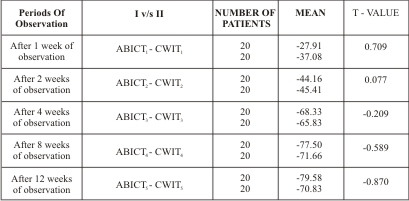
TABLE 3:
Showing the comparison of the reduction in mean percentage change in dentinal hypersensitivity at different periods of observation in category II and IV
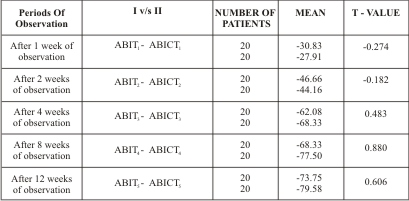
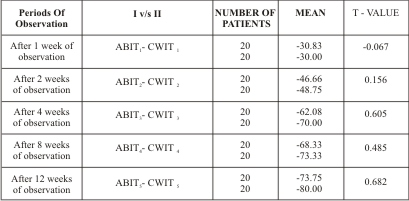
Table 4 & 5 (graph 4 & 5) shows that there was no statistically significant difference in reduction of dentinal hypersensitivity when compared between air blast stimulus and cold water stimulus. No worsening of scores from the baseline was observed at the end of the study.
TABLE 4:
Showing the comparison of the reduction in mean percentage change in dentinal hypersensitivity at different periods of observation in category I and II
TABLE 5:
showing the comparison of the reduction in mean percentage change in dentinal hypersensitivity at different periods of observation in category III and IV
The results further indicated that the improvement in dentinal hypersensitivity was statistically insignificant comparing two modes of stimuli i.e. air blast and cold water stimuli in both the groups. However, the improvement was statistically significant in group A and in group B i.e. subjects when treated with iontophoretic application alone and a similar application combined with coronally repositioned flap for both the stimuli.
DISCUSSION
The menace of dentinal hypersensitivity is one of the most common ailments confronted in routine by the dentists. Over the years, a wide variety of materials and methods4 have been tried for the treatment of dentinal hypersensitivity. Various agents have been used for the treatment of dentinal hypersensitivity with varying results. These agents include sodium fluoride12, stannous fluoride12, sodium monofluorophosphate13, strontium chloride6, sodium citrate14, potassium oxalate15, resins/adhesives15 etc. These agents have been utilized for topical application8 either as a home16 care measure or as an office procedure17.
Iontophoresis is one such procedure whereby the desensitizing agents are penetrated deep5 into the open dentinal tubules with the help of electric current. Recently, various periodontal surgical procedures are also being tried18 to cover the denuded root surface so as to alleviate the problem of dentinal hypersensitivity. Tarnow’s technique of covering of exposed root surfaces using a semilunar flap was described as a definitive treatment by Thompson19 for eliminating the dentinal hypersensitivity.
The present study was carried out to evaluate and compare the effect of iontophoretic application of 1 % sodium fluoride solution at 1 mA current for 1 minute on one side to the effect of a similar iontophoretic application combined with coronally repositioned flap on the other side in the management of dentinal hypersensitivity on exposed root surfaces.
Two stimuli in the form of air blast and cold water were used in the study to diagnose and evaluate the grade of dentinal hypersensitivity. Various techniques and methods have been tried in the past, but these two methods are easy to manipulate and are well accepted. (Gillam and Newman 1993)20.
The findings of the present study in group A (category I & II), showed marked improvement in almost 100% of the treated teeth. Patients remarked a significant reduction in dentinal hypersensitivity with sodium fluoride iontophoresis. These findings are in concurrence with findings of Jensen (1964)7, Murthy et al (1973)21, Carlo (1982)22, Lutins et al (1984)23, Kern (1989)8, Mc Bride et al (1991)24, who have also reported a variable but significant reduction in dentinal hypersensitivity with the use of fluoride iontophoresis. The findings of the study further indicated that the dentinal hypersensitivity decreased substantially with both the techniques employed i.e. iontophoresis with 1% sodium fluoride solution alone and a similar application combined with coronally repositioned flap procedure. However, when group A and B were compared, the decrease in dentinal hypersensitivity was not statistically significant after 12 weeks of observation showing thereby the iontophoretic application of 1 % sodium fluoride alone remarkably reduced the dentinal hypersensitivity. However the procedure when used in combination with coronally repositioned flap gave the additional benefit of a better esthetic appearance by covering the denuded root surfaces. Further, iontophoretic application of 1 % sodium fluoride at 1 mA current for 1 minute was considered safe since no untoward reaction was seen during the course of study. These findings are in concurrence with the findings of earlier studies viz Sausen (1955)25, Collins (1962)26, Scott (1962)27 and Lefkowitz (1962)28 who have shown the current upto 1 mA was safe to use as it had no adverse effect on pulpal tissue. No worsening of scores was observed at the end of the study.
The results further indicated that the improvement in dentinal hypersensitivity was statistically insignificant comparing two modes of stimuli i.e. air blast and cold water stimuli in both the groups. However, the improvement was statistically significant in group A and in group B i.e. subjects when treated with iontophoretic application of 1 % sodium fluoride solution alone and a similar application combined with coronally repositioned flap for both the stimuli.
One striking finding during study was that in all the four categories, a few patients showed an increased rating of hypersensitivity after being subjected to both the treatment modalities during the course of study. The fluctuation observed might be attributed to the lack in following the plaque control instructions, improper and forceful tooth brushing, intake of acidic food substances and psychological factors altering the pain reaction as reported in earlier studies by Addy, Absi and Adams (1987)29 and Curro (1990)2. The patients were motivated again to follow the proper oral hygiene measures and the treatment regimen meticulously.
Within all the four categories, it was found that there was a gradual increase in the percentage of teeth showing good relief over the passage of time and at 12 weeks of observation period, the sensitivity was decreased significantly as compared to the baseline scores. It might be attributed to the natural desensitization of dentin, iontophoretic application of sodium fluoride and coverage of denuded root surfaces by the coronal positioning of flap contributing to the reduction in dentinal hypersensitivity.
Several explanations are quoted in the literature for the natural desensitization of the denuded root surfaces. As saliva is saturated in calcium and phosphate with respect to most forms of insoluble calcium phosphate at normal salivary flow rates and pH, there are numerous physiochemical mechanisms tending to occlude dentinal tubules with a variety of crystal types. The transudation of plasma and the macromolecules that it contains may tend to fill the tissue spaces and perhaps the pulpal ends of tubules with fibrin, thereby decreasing the size of diffusion channels and decreasing dentinal permeability.
Although the exact mechanism by which fluoride iontophoresis produces desensitization is not known, several hypothesis have been proposed. One mechanism proposed28 involves the formation of reparative dentin following application of current to dentin which results in formation of dead tracts in the primary dentin. Another explanation of iontophoresis is that the electric current produces paraesthesia by altering the sensory mechanisms of pain conduction. A third alternative explanation is that the concentration of fluoride ions in dentinal tubules may be increased due to fluoride iontophoresis which could cause microprecipitation of calcium fluoride that may block hydrodynamically mediated pain inducing stimuli30. Another possible explanation is that fluoride ion has been demonstrated to be a potent inhibitor of many enzymes. It may be that intracellular changes in sensory nerves or other cells are responsible for interference of nerve conduction31.
The coronal positioning of the gingival tissue to correct root sensitivity is explained on the basis that the gingival tissues covering the denuded root surfaces tend to isolate the exposed dentin from the oral fluids and thermally insulate the area. The granulation tissue that fills the semilunar area turns into the same type of tissue that was present before repositioning of the tissue and usually of the similar color. This surgery also enhances gingival esthetics19.
CONCLUSION
The present study recommends the use of iontophoresis alongwith repositioning of flap to alleviate the menace of dentinal hypersensitivity and also to improve the esthetics of the patients. However, before some definitive conclusion can be drawn, further studies are warranted on larger number of samples using objective criteria of evaluation.
ACKNOWLEDGEMENTS
The author is grateful to Dr. Amarjit Singh Gill, Principal, Surendra Dental College, Ganga Nagar, for his valuable support, guidance and necessary facilities provided to carry out the study.
TABLES
The abbreviations used in tables and graphs are:
AB = Air-blast stimulus
CW = Cold water stimulus
I = Iontophoretic application of 1 % sodium fluoride solution at 1 mA current for
one minute
IC = Iontophoretic application of 1 % sodium fluoride solution at 1 mA current for
one minute combined with coronally repositioned flap procedure
T0 = Observation at preoperative level
T1 = Observation at 1 week of time interval
T2 = Observation at 2 weeks of time interval
T3 = Observation at 4 weeks of time interval
T4 = Observation at 8 weeks of time interval
T5 = Observation at 12 weeks of time interval
BIBLIOGRAPHY
1. Gorman WJ. Prevalence and etiology of gingival recession. J.Periodontol 1967;38:316.
2. Curro FA, Ed. Tooth hypersensitivity. Dent Clin North America 1990;34(3):403-587.
3. Reinhart TC, Killoy WJ, Love J, Overman PR, Sakumara JS. The effectiveness of a patient applied tooth desensitizing gel: A pilot study. J Clin Periodontol 1990;17:123-127.
4. Berman LH. Dentinal sensation and hypersensitivity: A review of mechanisms and treatment alternatives. J Periodontol 1984;56(4):216-222.
5. Wilson JM, Fry BW, Walton RE, Gangarosa LP. Fluoride levels in dentin after iontophoresis of 2 % sodium fluoride. J Dent Res 1984;63(6):897-900
6. Gupta RR. To compare the effect of the strength of electrical; current in the management of dentinal hypersensitivity with iontophoretic unit using 10 % strontium chloride, MDS thesis, Pbi Univ, Patiala, 1994.
7. Jenson AL. Hypersensitivity controlled by iontophoresis – Double blind clinical investigation. J Am Dent Assoc 1964;68:216-224.
8. Kern DA, McQuade MJ, Scheidt MJ, Hansen B, Van Dyke TE. Effectiveness of sodium fluoride on tooth hypersensitivity with or without iontophoresis. J Periodontol 1989;60:386-389.
9. Barbakow F. Investigations of the effect of iontophoresis on the surface fluoride content in enamel. J Dent Res 1972;51:845.
10. Sumner CF. Surgical repair of recession on the maxillary cuspid : Incisally positioning the gingival tissue. J Periodontol 1969;55:119-121.
11. Restrepo OJ. Coronally repositioned flap : Report of four cases. J Periodontol 1973;44(9):564-568.
12. Addy M, Mostafa P. Dentin hypersensitivity – Part II. Effects produced by the uptake invitro of tooth pastes on to dentin. J Oral Rehab 1989;16:35-48.
13. Bansal M. Comparison of efficacy of 1 % solution of sodium fluoride, freshly prepared and commercially available (Flucol Solute) in the management of dentin hypersensitivity, MDS Thesis, Pbi Univ, 1999.
14. Tarbet WJ, Silverman G, Fratarcangelo PA, Kanapka JA. Home treatment for dentinal hypersensitivity – A comparitive study. J Am Dent Assoc 1982;105:227-230
15. Johnson RH, Zulqar Nain BJ, Koval JJ. The effectiveness of an electroionizing tooth brush in the control of dentinal hypersensitivity. J Periodontol 1982;53:353-359.
16. Wycoff SJ. Current treatment for dentinal hypersensitivity, Comp Cont Educ Com Dent (suppl. 3), 1982. Quoted by Reinhart TC et al. The effectiveness of a patient applied tooth desensitizing gel. J Clin Periodontal 1990;7:123-127.
17. Welch EH, Eick JD. A method to reduce or prevent post operative sensitivity with posterior composite resin restorations. Quintess Int 1986;7:667-676.
18. Prato GP et al. Guided tissue regeneration versus mucogingival surgery in the treatment of human buccal gingival recession. J Periodontol 1992;63:919-927.
19. Thompson BK, Meyer R, Singh GB, Mitchel W. Desensitization of exposed root surfaces using a semilunar coronally repositioned flap. Gen Dent 2000;68-71.
20. Gillam DG, Newman HN. Assessment of pain in cervical dentinal sensitivity studies : A review. J Clin Periodontol 1993;20:383-394.
21. Murthy KS, Salim ST, Singh I. A comparative evaluation of topical application and iontophoresis of sodium fluoride for desensitization of hypersensitive dentin. J Oral Surg 1973;36:448-458.
22. Carlo GT, Ciancio SG, Seyrek SK. An evaluation of iontophoretic application of fluoride for tooth desensitization. J Am Dent Assoc 1982;105:452-454.
23. Lutins ND, Grecot GW, McFall WT. Effectiveness of sodium fluoride on tooth hypersensitivity with or without iontophoresis. J Periodontol 1984;55:285-288.
24. McBride MA, Gilpatrick RO, Fowier WI. The effectiveness of sodium fluoride iontophoresis in patients with sensitive teeth. Quintess Int 1991;22:637-640.
25. Sausen R. Electrophoresis in dentine with radioactive calcium. J Dent Res 1955;34:12.
26.Collins EM. Desensitization of hypersensitive teeth. Dent Digest 1962;360-363.
27. Scott HM. Reduction of sensitivity by electrophoresis. J Dent Child Fourth Quarter, 1961;225-241.
28 Lefkowitz W. Pulp response to ionization. J Prosthet Dent 1962;12(5):966-976.
29.Addy M, Absi EG, Adams D. Dentin hypersensitivity – The effects in vitro of acids and dietary substances on root planed and burred dentin. J Clin Periodontol 1987;14:274-279.
30 Gangarosa LP (Sr), Park NH. Practical considerations in iontophoresis of fluoride for desensitizing dentin. J Prosthet Dent 1978;39:173.
31 Walton RE, Leonard LA, Sharawy M, Gangarosa LP, Augusta GP. Effects on pulp and dentin of iontophoresis of sodium fluoride on exposed roots in dogs. J Oral Surg 1977;48:545-556. |