Introduction
Pulp necrosis is a common sequela following traumatic injuries to teeth[1]. The necrosis of pulp may be followed by arrested tooth development and subsequently, infection of the root canal and peri-radicular tissues with or without sinus tract formation. When the pulp undergoes pathologic changes before root canal is completed, dentin formation ceases and root growth is arrested[2]. In such circumstances, endodontic treatment becomes challenging as the walls of the root canals are frequently divergent making debridement and obturation difficult[3]. In addition, because of thin dentinal walls, these teeth are susceptible to fracture after treatment.
Before 1966, the clinical management of the "Blunder buss" canal usually required a surgical approach for the placement of an apical seal into the often fragile and flaring apex. The treatment was complicated when patient management required conscious sedation or general anaesthesia, especially with children. The apexification with calcium hydroxide has proved to be a reliable and most welcome addition to the therapeutic armamentarium since Frank described it in 1966[4].
Here we present four cases of teeth with open apices and necrotized pulps where apical barrier formation was induced by Ca(OH)2.
Case reports
Case 1
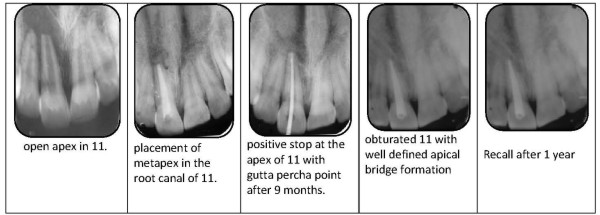
A 10-year-old male patient was reported to the paediatric dental clinic complaining of an intense pain, swelling & draining sinus in maxillary anterior region. The history revealed trauma 6 months previously during a fall. On clinical examination, a draining sinus was found on the labial aspect of right central incisor. The tooth was tender to percussion test and it was negative to pulp sensitivity tests. Radiographically, wide open apices with divergent canal walls and periapical radiolucency was evident. A diagnosis of pulp necrosis with chronic periapical abscess w.r.t 11 was established.
Case 2
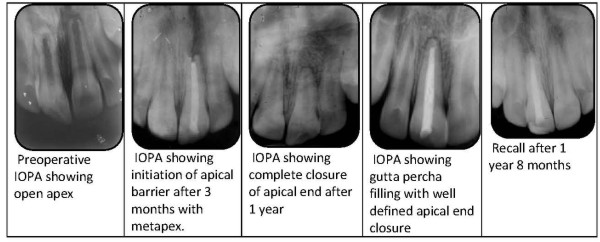
A 9.5 year male patient was referred to our clinic for endodontic treatment of his left maxillary central incisor. There was a history of trauma with an un-complicated fracture of incisal edge. The tooth was clinically asymptomatic. There was no intraoral sinus tract related to involved tooth. The vitality tests with thermal and electric pulp testing gave a negative response. IOPA revealed peri-radicular radiolucency in relation to 21 and wide open apex.
Case 3
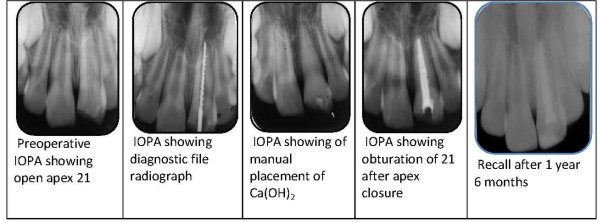
A 9 year old boy reported to the department with a chief complaint of intermittent pain in upper front tooth which had increased intensity for the past 1 week. The patient gave a history of trauma 1 month earlier wherein there was a direct impact on maxillary anteriors. There was no apparent swelling in relation to the involved tooth. No periodontal pockets were present and thermal and electric pulp testing elicited negative response. Radiographically, the tooth exhibited incomplete root formation, characterized by a wide root canal.
Case 4
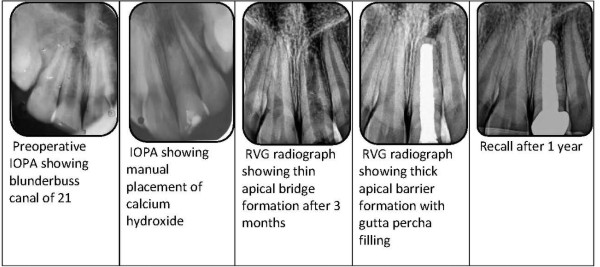
A 10 year old boy came to the dental clinic with a chief complaint of fractured left central incisor. The injury occurred at school while he was playing and he reported to the dental clinic after a week. The vitality test with thermal and EPT elicited negative response. In the preoperative radiograph, the root apex had incomplete root formation with apical radiolucency.
 | Case 1
 |
 | Case 2
|
 | Case 3
|
 | Case 4
|
In all the above mentioned cases, the involved teeth were immature teeth with open apices, hence apexification with the help of Ca(OH)2 was performed.
In the procedure, after rubber dam application, access opening was performed and a diagnostic file radiograph was taken to establish working length. The debridement was carried out by gentle filing and irrigation, using 3% sodium hypochlorite and saline alternately. A CMCP (camphorated monochloro phenol) open dressing was placed when there was acute infection and a closed dressing was given when the tooth was asymptomatic. The patient was prescribed antibiotics and analgesics in case of infection. Subsequently, a calcium hydroxide paste was pushed either manually (Cases 3 & 4) or with the help of preformed syringes (Cases 1 & 2 with metapex syringe). If there was recurrence of pain and swelling after pushing the Ca(OH)2, the procedure was repeated similarly. The Ca(OH)2 was kept in the root canals for at least 6 months and if needed, it was changed accordingly. On routine radiographic examination, it was revealed that there was complete closure of the apices of all teeth. In some cases, there was complete resolution of the periapical radiolucencies (Cases 1 & 4).
Discussion
Apexification is defined as the process of creating an environment within the root canal and periapical tissues after pulp death that allows a calcific barrier to form across the open apex of an immature root (Pitt Ford 2002). This barrier has been characterized as dentin, cementum, bone, osteocementum and osteodentin. The result is blunting of the root end and very little, if any, increase in root length[4].
The apical closure of blunder buss canals have been reported by Frank in 1966 to be of four types as seen clinically as well as in the radiographs. These are: 1) normal closure of apex with continued root formation, 2) dome-shaped apical closure with the canal retaining a blunderbuss appearance, 3) there is positive stop but no evidence of apical closure radiographically and 4) there is a positive stop with radiographic evidence of a barrier coronal to the anatomic apex of the tooth[5].
There are numerous procedures and materials recommended to induce root-end closure in teeth with immature apices. These procedures include:
1. only Ca(OH)2 or Ca(OH)2 mixed with various materials[6].
2. mineral trioxide aggregate (MTA)[7],
3. infection control[8],
4. induction of a blood clot in the periradicular tissue[9],
5. antibiotic pastes[10],and
6. no treatment[11]
However, Ca(OH)2 remains a popular material to accomplish apical closure due to its apparent ability. This is because of its high alkalinity and bactericidal effect. It is also reported to stimulate alkaline phosphatase activity. The medicament is also easy to manipulate into the root canals. It is also easily available and inexpensive. Recently, MTA is becoming more popular but when compared to Ca(OH)2, it is expensive and the technique is more difficult to place the material into the root canal.
The apexification procedures and its results using Ca(OH)2 were reported by various authors throughout the world. The medicament (Ca(OH)2) can be used in combination with sterile water, saline, local anesthetic, camphorated parachlorophenol, zinc oxide paste with cresol and iodoform[12], polyantibiotic paste[13] and tricacium phosphate[14]. Chawla and Tewari 1980 reported that apexification can be induced with calcium hydroxide without a catalyst[15]. Gutman and Heaton in 1981, reported that the addition of other medicament to Ca(OH)2 has no beneficial effect on apexification[16]. Cvek (1972) observed apical root closure and bone healing following intracanal placement of Ca(OH)2 in 50 of 55 maxillary incisors with immature roots[17]. Furthermore, Binnie and Rowe (1973) dressed immature premolars in dogs with Ca (OH)2 and distilled water and observed a minimal inflammatory response in the periapical tissues with continued root formation[18].
Conclusion
In this present investigation, the apex closure was observed in 6-18 months period using Ca(OH)2. We found that there was no differences using Ca(OH)2 without any medicament and a combination of Ca(OH)2 with iodoform (metapex). It was also observed that there was no difference between manual pushing of Ca(OH)2 with hand instrument and using readymade Ca(OH)2 syringes (metapex).
References:
1. Gamze Erdogan. The treatment of non-vital immature teeth with calcium hydroxide-sterile water paste: Two case reports. Quintessence International 1997; 28 (10) : 681-86.
2. Barnett F. The role of endodontics in the treatment of luxated permanent teeth. Dental Traumatology 2002; 18 : 47-56.
3. Sheehy EC. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: a review. British Dental Journal 1997; 183 : 241-46.
4. Anantharaj A ,Praveen P, Karthik Venkataraghavan, Prathibha Rani S, Sudhir R,Murali Krishnan B. Cchallenges in pulpal treatment of young permanent teeth - A Review. Journal of Dental Sciences and Research. 2011; 2: 142- 155.
5. MCDONALDS
6. Frank A. Therapy for the divergent pulpless tooth by continued apical formation. J Am Dent Assoc 1966;72:87-93.
7. Walton RE, Torabinejad M. Management of incompletely formed roots. In: Principles and Practice of Endodontics. 3rd ed. Philadelphia, Pa: WB Saunders; 2002:388-404.
8. Das S. Apexification in a nonvital tooth by control of infection. J Am Dent Assoc 1980;100:880-881.
9. Ham J, et al. Induced apical closure of immature pulpless teeth in monkeys. J Oral Surg 1972;33:438-448.
10. Ball JS. Apical root formation in a non-vital immature permanent incisor. Br Dent J 1964;116:116-117.
11. Lieberman J, Trowbridge H. Apical closure of nonvital permanent incisor teeth where no treatment was performed: Case report. J Endod 1983;9:257-260.
12. Cooke C, Rowbotham TC. 'The closure of open apices in nonvital immature incisor teeth'. Br Dent J. 1988;165:420-1.
13. Rule DC, Winter GB. Root growth and apical repair subsequent to pulpal necrosis in children. Br Dent J. 1966;120:586-90.
14. Coviello J, Brilliant JD. A preliminary clinical study on the use of tricalcium phosphate as an apical barrier. J Endod. 1979;5:6-13.
15. Chawla HS, Tewari A, Ramakrishnan E. A study of apexification without a catalyst paste. J Dent Child 1980;47:431-4.
16. Gutmann JL, Heaton JH. Management of the open (immature) apex and non-vital teeth. Int End J. 1981; 14: 173-7.
17. Cvek M. Treatmet of non-vital permanent incisors with calcium hydroxide and follow - up of periapical repair and apical closure of immature roots. Odontologisk Revy.1972; 23: 27-44.
18. Binnie WH, Rowe AH. A histological study of the periapical tissues of incompletely formed pulpless teeth filled with calcium hydroxide. J Of Dent Res. 1973; 52:1110-6. |