Introduction
Resorption of alveolar bone following loss of teeth is an inevitable outcome. In cases with trauma or congenital defects, this resorption is further increased. Prosthodontic treatment of such large anterior ridge defects requires not only replacement of the missing teeth but also the restoration of the bone defect, esthetics and phonetics. This situation can pose quite a challenge to the clinician. The term localised alveolar ridge defect is intended to refer to volumetric deficit of limited extent in bone and soft tissue within the alveolar process.[1] Such large defects may require surgical correction before prosthetic treatment.[2]Previous researchers have classified these defects both qualitatively and quantitatively.[3],[4]
Classification of the ridge defects
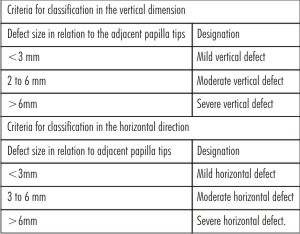
The most commonly used classification is the Seibert’s nomenclature. It classifies the defects from Class I to Class III.[3](Table 1) Another classification was given by Allen[3] that classifies the defects from Type A to Type C.[4] (Table 1) However, these classifications do not describe the dimension of the ridge defect quantitatively. For this reason, a more detailed classification was proposed.[1] According to this classification, a semiquantitative analysis of severity of bone loss in vertical and horizontal
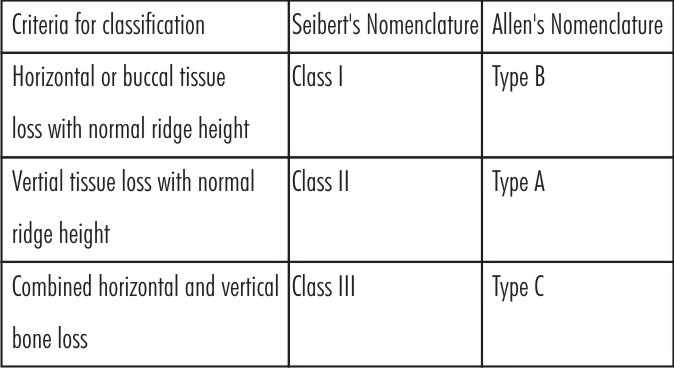 | Table 1: Classification of the anterior ridge defects.
 |
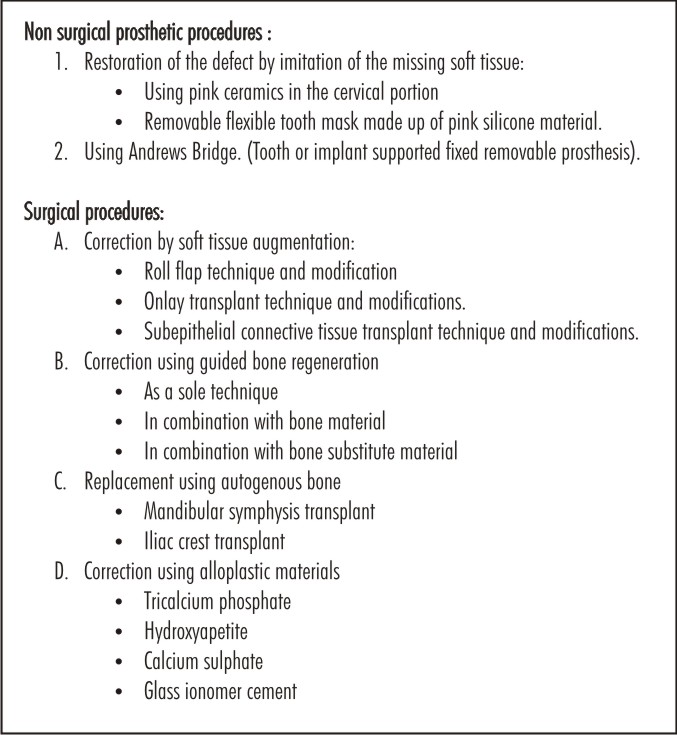
 | Table 2: Surgical and non-surgical procedures of correcting the anterior ridge defects
|
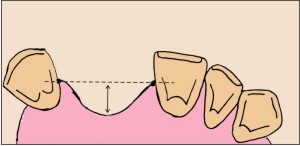
direction was done. Based on this classification, the vertical component of the defect is measured from the deepest point of the defect and an imaginary dental arch running through the tips of the papillae of the adjacent teeth. (Fig.1)
The horizontal component is measured as the distance between the deepest point of the defect and an imaginary dental arch line running over the bucco-gingival margin and the cemento-enamel junction of both the adjacent teeth. (Fig. 2, Table 2).
The pre-operative classification of a ridge defect according to its expanse, its severity and its form is clinically relevant because such classification permits the establishment of a preliminary prognosis for a planned restoration.
These defects may be restored in principle by two methods: the defect may be corrected surgically during the pre-prosthetic phase, or it may be restored nonsurgically using fixed and or removable prosthesis. The options of surgical and prosthodontic treatment is
 | Table 3: Semiquantitative classification of localised alveolar defect.
|
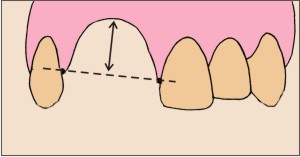 | Fig 1: Semi quantitative measurement of the vertical component.
|
 | Fig 2: Semi quantitative measurement of the horizontal component.
|
 | Fig 3: Pre-operative view.
|
The classification helps to the estimate the surgical and technical difficulties of the procedure. It has been seen that the vertical component of the ridge defect is more difficult to reconstruct than the horizontal component.
Prosthetic treatment of a surgically uncorrected localized alveolar ridge defect with a fixed restoration is associated with several esthetic challenges like loss of papillae and formation of open “black” interdental spaces; compromised phonetics due to open space; danger of food impaction under the pontic; loss of buccal contour and many more.[2] In large defects, the treatment options like fixed/ implant prosthodontics are unable to fulfill all the requirements. In such conditions, the Andrewsbridge is a good prosthodontic option. It was Dr. James Andrews of Amite, Louisiana who introduced fixed-removable Andrews System (Institute of Cosmetic Dentistry, Amite, L.A.).[5] He developed this technique to overcome the problems associated with the restorations of severe residual ridge resorption or jaw defect cases.
Following are the clinical situations in which Andrews bridge System can be considered:
1) Excessive residual ridge defect.
2) Ridge defects/ jaw defects either due to trauma and/or surgical ablation.
3) Cleft lip/palate patients with congenital or acquired bone defects.[6]
4) In patients with periodontal problems.[6]
The advantages of Andrews Bridge are:
a) It includes all the advantages of fixed and removable partial dentures with better aesthetics, hygiene along with better adaptability and phonetics.
b) Absence of palatal coverage increases patient comfort.
c) It is economical treatment option for the patient.
Two types of the Andrews System has been described. It can either be supported by natural teeth as abutments or it can be supported with the help of implants.
This article explains the procedure of fabricating and correcting an anterior ridge defect using a tooth supported fixed-removable Andrews Bridge.
Case Report:
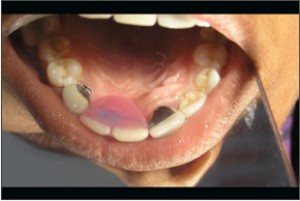
An 18-year-old girl reported to the Department of Prosthodontics with the chief complaint of dissatisfaction with the appearance of front teeth. The patient gave the history of surgical correction of cleft palate six months ago. Upon further evaluation, it was evident that there was rotated tooth no.11, peg shaped tooth no.12 and a supernumerary tooth present between 12 and 13. On further evaluation it was found that 11, 12 and the supernumerary tooth had Grade II mobility.(Fig. 3) The periapical radiograph of the patient showed that there was large amount of angular bone loss in the above mentioned area. On further discussion, the patient expressed her strong refusal to undergo any surgical procedures.
Treatment Plan
The rotated and mobile teeth (no.11, 12) and the supernumerary tooth were decided to be extracted. Following extraction and healing of the socket, the defect in the bone was clearly evident. The defect was classified to be Class III according to Seibert's Classification and Type C according to Allen's nomenclature. On measuring the defect, it was found to have a severe vertical defect >6 mm and severe horizontal defect >6 mm. A Class III bone defect results in a large three sided defect making placement of graft material and implants questionable. It was thus decided to fabricate an Andrews fixed removable prosthesis for the restoration of the missing teeth and for the closure of the bone defect.
Alginate (Tropicalgin, Zhermac) impressions were made of the maxillary and the mandibular arches. A wax-up with the removable partial denture was done such that the partial denture would restore the esthetics and closure of the defect. The try-in of the removable partial denture was done to check for the esthetics and phonetics. A putty index of the trial denture was made.
The abutment teeth 21 and 13 were prepared to receive Porcelain fused to metal (PFM) crowns. Elastomeric impressions were made using polyvinylsiloxane (Aquasil Putty Material, Dentsply) and master casts were poured in dental stone (Type IV, Ultrarock Kalabhai). Removable dies were prepared and the wax patterns of the copings were fabricated. Pre-fabricated plastic bar attachment (OT Bar Multiuse, Rhein 83) was attached according to the ridge form. Putty index was placed on the cast to check for the correct positioning of the bar. (Fig. 4) The bar along with the copings was casted in cobalt chromium alloy. The metal framework was tried in to check for the esthetics, phonetics and proper hygienic access of the area. (Fig. 5) Shade selection was done and ceramic firing was done on the copings. After finishing and polishing, the cementation of the PFM crowns along with the bar was done with glass ionomer cement (GC Fuji I). (Fig 6) With the crowns cemented in place, alginate (Tropicalgin, Zhermack) impressions were made and stone cast was poured. The missing teeth were arranged in the wax rim and trial was done. Acrylisation (Trevalon HI, Dentsply) was done with the clip in the lingual aspect. (Fig. 7) The removable portion was then attached over the bar attachment. (Fig. 8 & 9)
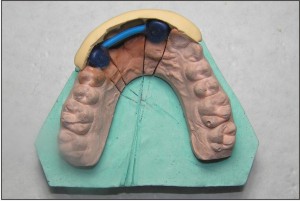 | Fig 4: Wax pattern of the bar with the putty index.
|
 | Fig 5: Try-in of metal framework of the bar and the copings.
|
 | Fig 6: Cemented PFM crowns with the attached bar.
|
 | Fig 7: Acrylised removable component with the sleeve.
|
 | Fig 8: Intra oral view of the removable component placed over the bar.
|
 | Fig 9: Palatal view of the removable component in place with complete defect closure.
|
The patient was trained to place and remove the removable component fabricated over the fixed component of Andrews Bridge and proper oral hygiene instructions (including interdental brush)were given to the patient. Periodic recall was done to check for the adaptability and assess the success of the final prosthesis.
Discussion
Clinicians often come across clinical situations with localised alveolar ridge defects. It has been reported that only 9% of the patients with the anterior teeth missing between the two canines did not have ridge defects.[7] The most commonly seen defects are the combined Class III defects (56% of cases) followed by horizontal defects Class I (33% of the cases).[7] Vertical defects were reported to be found in 3% of the patients.[8] Large vertical and horizontal bone defects pose a prosthodontic challenge as it is difficult to restore esthetics and function along with the complete closure of the defect. Such clinical conditions are not successfully treated by conventional fixed or removable prosthesis.
Recently, spark-erosion technology has been introduced in dentistry. It is made of a primary bar casting joining the implants and a removable metal superstructure upon which the replacement teeth are processed. The precise fit of the secondary restoration over the primary bar casting and the rigid fixation with the spark eroded attachment dictate that the restoration becoming viewed as totally implant supported. Both the Andrews bar system and the spark-erosion overdenture share the similarity of having the advantages of the totally implant supported fixed partial denture and the implant supported overdenture.[9] However, the inherent problems associated with the fabrications of spark-erosion overdenture may limit the availability of the technology to the profession because they require high laboratory precision, are bulky and tend to wear out.
Surgical correction of the defects using grafts and placement of implants is an expensive treatment plan for some patients. Surgical procedures also require patient's consent. In conditions where conventional removable or fixed is not a feasible option as in the case presented above;a third treatment option of functionally fixed partial dentures can prove successful in restoring function, esthetics, speech and closure of the defect.
Limited reports of the failure of such prosthesis are found in the literature. The failures are mainly due to inadequate soldering. However, this was completely eliminated by attaching retainers to the bar in a single casting.[10] The patient was recalled and evaluated over a period of two years. The patient was comfortable and happy with the final outcome and had pleasing aesthetics and phonetics.(Fig 10)
 | Fig 10: Post-operative view.
|
Conclusion
Andrews Bridge System is a fixed-removable prosthesis that is indicated in patients with large ridge defects. The functionally fixed prosthesis successfully replaces the missing teeth along with complete closure of the defect, restores speech and esthetics.
References:
1. Studer S, Naef R, Scharer P. Adjustment of localized alveolar ridge defects by soft tissue transplantation to improve mucogingival esthetics: A proposal for clinical classification and evaluation of procedures. Quintessence Int 1997;28(12):785-805.
2. Seibert JS, Cohen DW. Periodontal Considerations in preparation for fixed and removable prosthodontics. Dent Clin North Am 1987;31(3):529-55.
3. Seibert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent 1983;4(5):437-53.
4. Allen EP, Gainza CS, Farthing GG, Newbold DA. Improved technique for localised ridge augmentation. A report of 21 cases. J Periodontol 1985;56(4):195-9.
5. Everhart R, Cavazos E. Evaluation of fixed removable partial denture: Andrews bridge system. J Prosthet Dent 1983;50(2):180-84.
6. Stein RS. Pontic - residual ridge relationship: A Research Report. J Prosthet Dent 1966;16(2):251-85.
7. Abrams H, Kopczyk RA, Kaplan AL. Incidence of anterior ridge deformities in partial edentulous patients. J Prosthet Dent 1987;57(2):191-4.
8. Garber DA, Rosenberg ES. The edentulous ridge in fixed prosthodontics. Compend Contin Edu 1981;2(4):212-23.
9. Salinas TJ, Finger IM, Thaler JJ 2nd, Clark RS. Spark-erosion implant supported overdentures : clinical and laboratory techniques. Implant Dent 1992;1(4):246-51.
10. Chandra S, Ajay S, Gupta H, Chandra C. Treatment using functionally fixed prosthesis: A case report. J Indian Prosthodont Soc. Doi 10.1007/s13191-013-0258-6 |