Introduction
A thorough knowledge and understanding of the root canal anatomy and anticipation of their possible morphological aberrations is an essential prerequisite for successful endodontic management. The inability to recognize and prepare all canals of the endodontic system may be a major cause of the failure of endodontic therapy. Although all teeth may present anatomical variations, the “6-year molar” or the mandibular first molar is the first permanent posterior tooth to erupt and most often suffer from caries and is likely to undergo endodontic treatment.[1] The mandibular first molar usually has two canals in the mesial root and one/two canals in the distal root[2] but numerous variations regarding the root canals in this tooth are extensively reported.[3],[14] The incidence of a third canal in the distal root is as low as 3%.[3]
The purpose of the present article is to report the successful non-surgical endodontic management of a permanent mandibular first molar having three distal root canals with the aid of the operating microscope.
Case Report
A 28-year old female patient was referred to our department with a chief complaint of pain in lower right back tooth region for the past 3 days. Patient’s medical history was non-contributory. Dental history revealed that the patient had undergone incomplete endodontic
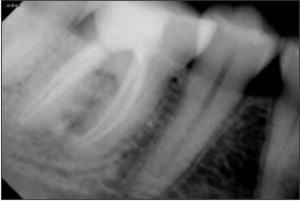
therapy by a private practioner 1 year previously. Clinically, the tooth #46 showed a fractured distoocclusal temporary restoration. A pre-operative diagnostic radiograph revealed occlusal radiolucency suggestive of dental caries around the temporary restoration. The pulp chamber was already open (Fig. 1). From the preoperative examination and radiographic findings a diagnosis of nonvital tooth with symptomatic apical periodontitis was made for the tooth #46 and non-surgical endodontic treatment was planned.
The tooth was isolated with rubber dam and cotton rolls. Temporary restoration and secondary caries was removed. Acess opening was modified. The pulp chamber was examined under an operating microscope (Gem Optical Instrument Industries; HSIDC, Ambala Cantt, India). Observation of the pulp chamber under magnification 14 X with the aid of the operating microscope revealed another root canal orifice inbetween distolingual and distobuccal canal. Five canals identified were: mesiobuccal (MB), mesiolingual (ML), distobuccal (DB), middle distal (MD), distolingual (DL). Coronal flaring was carried out with Gates Glidden drills (Fig. 2) and working length was determined with the help of an apex locator (Root ZX; Morita, Tokyo, Japan), which was later confirmed with a radiograph (Fig. 3).
 | Fig 1. Pre operative radiograph of tooth 46
 |
 | Fig 2. Clinical view of the pulp chamber floor with the aid of the operating microscope under magnification 14.2 X showing 5 canals: mesiobuccal MB, mesiolingual ML, distolingual DL, distobuccal DB and middle-distal MD.
|
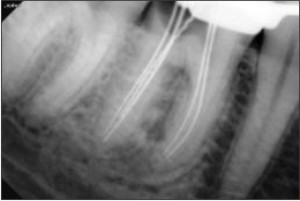 | Fig 3. working length determination
|
 | Fig 4.Final Post operative radiograph
|
 | Fig 5. One-year recall radiograph of tooth 46
|
The pulp chamber was again examined
imagined but also something that can be approached visually.
The use of magnification and fiberoptic illumination helps in locating and negotiating extra root canals [15]. The surgical operating microscope has been found to be particularly useful because it gives the clinician the opportunity to improve the optical field and to distinguish microstructures that are not distinct with the naked eye.[16]
Conclusion
This case underscores the importance of thorough inspection of the floor of pulp chamber to detect all the root canal orifices. Each case should be cautiously examined and the clinician should develop skills necessary to detect any possible variation the root canal system for long-term successful endodontic therapy. Apart from clinical and radiographic examination, enhanced illumination and visibility with an operating microscope should be considered to ensure predictable and successful results. The present case contributes to our knowledge of the anatomical aberrations that occur in mandibular first molar.
References
1. Cohen S, Hargreaves KM. Pathways of the pulp. 9th ed. Louis; Mosby: 2005:220
2. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1984;58:589-99.
3. Ahmed HA, Abu-bakr NH, Yahia NA, Ibrahim YE. Root and canal morphology of permanent mandibular molars in a Sudanese population. Int Endo J 2007;40:766-71.
4. Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: A case report and literature review. J Endod 2004;30:185-6.
5. Chandra SS, Rajasekaran M, Shankar P, Indira R. Endodontic management of a mandibular first molar with three distal canals confirmed with the aid of spiral computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009:108:e77-81.
6. Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod 1985;12:568-72.
7. Mushtaq M, Farooq R, Rashid A,
Cuxhaven, Germany) was applied, and temporary access was sealed with Cavit (3M ESPE AG, Seefeld, Germany). The patient returned after 2 week. The tooth was completely asymptomatic. Calcium hydroxide paste was removed, and root canals were obturated by cold lateral compaction of gutta-percha using zinc oxide and eugenol sealer (Kemdent; Associated Dental Products Ltd, Wilt- shire, UK). A postoperative final radiograph was taken (Fig. 4), and the access was restored permanently with universal composite resin restorative material (3M ESPE Dental Products, St Paul, MN). One-year recall radiograph showed satisfactory healing (Fig. 5).
Discussion
A successful endodontic treatment depends on the complete debridement and obturation of the root canal system. Inadequate cleaning and shaping of the root canal is considered to be one of the most important factors for endodontic failure. Hence, it is of utmost importance that all the canals be located and treated during the course of nonsurgical endodontic therapy. Usually, mandibular first molar presents with two root canals in the mesial root and one/two root canals in the distal root.[2] Presence of a third root canal in the distal root of mandibular molars is known as “middle distal canal”. This third canal is situated in the centre of buccal and lingual canals and is smaller than the other two canals. The etiology behind such canal system is still unclear but it is postulated that during tooth formation the secondary dentin apposition forms vertical dentinal partitions, thereby creating root canals.[12]
The occurrence of third canal in the distal root of first mandibular molar is rare. It ranges from 0.2%-3% [13] depending on the population variance and is reported to be 1.7% in an Indian population.[14] In this case, the presence of a missed and incompletely obturated root canal could have probably led to the persistence of clinical symptoms and subsequent failure of endodontic therapy.
Microscopes have been used for decades in various medical specialties and have recently been introduced to endodontics because of its inherent advantages including enhanced visibility and illumination. In this age of microscope-assisted endodontics, root canal vaiation is not only something that can be
under the operating microscope for additional canals, and further photographs were taken under magnification 10.0, 14.5, and 20.8 from different observation angles. The three distal root canal orifices were observed in an almost straight line.
The root canals were cleaned and shaped with Protaper (Dentsply, Maillefer, Ballaigues, Switzerland) rotary instruments under copious irrigation with 2.5% sodium hypochlorite and 17% ethylenediaminetetraacetic acid. The finishing of canals was performed until Protaper F2 reached the full working length. After preparation, the root canals were irrigated with 17% ethylenedia minetetraacetic acid and 2.5% NaOCl to remove the smear layer. The root canals were dried with sterile paper points (Dentsply, Maillefer). Calcium hydroxide paste (Calcicur; VOCO,
Endod 2011;37:878-80.
11. Stroner WF, Remeikis NA, Carr GB. Mandibular first molar with three distal canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1984;57:554-7.
12. Martinez-Berna A, Badanelli P. Mandibular first molars with six root canals. J Endod 1985:11;348-52.
13. Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: A case report and literature review. Int Endod J 2010;43:714-22.
14. Goel NK, Gill KS, Taneja JR. Study of root canals configuration in mandibular first permanent molar. J Indian Soc Pedod Prev Dent 1991;8:12-4.
15. Saunders WP, Saunders EM. Conventional endodontics and the operating micro- scope. Dent Clin North Am 1997;41:415-28.
16. Koch K. The microscope: its effect on your practice. Dent Clin North Am 1997;41:619 -26.
Source of Support : Nill, Conflict of Interest : None declared
Robbani I. Spiral computed tomographic evaluation and endodontic management of mandibular first molar with three distal canals. J Conserv Dent 2011;14:196-8.
8. Quackenbush LE. Mandibular molar with three distal root canals. Endod Dent Traumatol 1986;2:48-9.
9. Reeh ES. Seven canals in a lower first molar. J Endod 1998;24:497-9.
10. Ryan JL, Bowles WR, Baisden MK, McClanahan SB. Mandibular first molar with six separate canals. J |