Introduction:
Supernumerary teeth are described as the teeth formed in excess of the normal dental formula.[1] 90% of all supernumerary teeth are found in the anterior region of maxilla. Supernumerary teeth in the anterior mandible are not common and only account for about 1% of all supernumerary teeth.[2] This paper reviews the literature and reports a case of eumorphic supernumerary mandibular incisor erupted medially, causing crowding and aesthetic problems.
Literature Review
The first report of supernumerary teeth (hyperdontia) appeared between 23 to 79 AD.[3]There are various theories regarding the origin of supernumerary teeth; unknown etiology, continued budding of the dental lamina, proliferation of the remains of dental lamina, dichotomy, atavism, genetics and a combination of genetic and environmental factors.[4] Based on the present knowledge it is believed that hyperdontia is a multifactorial inheritance disorder that originates from hyperactivity of the dental lamina. [1]
Supernumerary teeth may be classified on the basis of position or morphology. [5] Positional variations include mesiodens, paramolars, distomolars and parapremolars. Primosch classified supernumerary teeth according to morphology as supplemental or rudimentary. A eumorphic or supplemental supernumerary tooth is similar morphologically to normal tooth while dysmorphic or rudimentary teeth are small and conical or tuberculate. [6],[7]
Supernumerary teeth may be single or multiple, unilateral or bilateral, and in one or both jaws. Single supernumeraries occur in 76 to 86% cases, double supernumeraries in 12 to 23% and multiple supernumeraries in less than 1% of cases. [8] Multiple supernumerary teeth are often found in syndromes such as Cleidocranial dyostosis, Gardener's syndrome and cleft lip and palate.
Anterior maxillary region appears to be the site of predilection for supernumeraries. A slight difference in the relative frequency of different supernumerary teeth has been reported in the literature but most authors are of the view that the maxillary midline supernumeraries are the most common type, followed by maxillary lateral incisor, mandibular third premolars, mandibular fourth molars and maxillary paramolars.[1] Luten's study suggests that 97% supernumeraries are located in anterior region. [9]
However, the occurrence of a supernumerary tooth is very rare in the incisor region of the mandible. Tanaka reported the first case of bilateral, completely erupted supernumerary teeth for mandibular incisors in Japan.[10] Bodin et al examined 21,609 patients and found 422 supernumerary teeth, of which only four were seen in mandibular incisor region.[11] Locht studied the radiographs of 704 children and found no case of supernumerary teeth in anterior part of mandible. [12]
The prevalence of supernumerary teeth varies from 0.15-3.8% in the permanent dentition.[2],[4],[9] The occurrence of supernumerary teeth in the primary dentition is a less common finding, one fifth of that seen in permanent dentition.[13]
No significant sex distribution of primary supernumeraries has been reported while in the permanent dentition the male-female ratio is 2:1.[1],[11]A study of Asian school children found a greater male to female distribution of 5.5:1 for Japanese and 6.5:1 for Hong Kong children.[8]
Effects of supernumerary teeth on the developing dentition vary. There may be no effect, with the supernumerary tooth being discovered either as a chance radiographic finding or following their eruption. Many complications have been associated with supernumeraries however, including impaction, delayed eruption or ectopic eruption of adjacent teeth, crowding, development of midline diastema, eruption into the floor of the nasal cavity, formation of dentigerous cyst and root resorption of adjacent teeth. [1],[5],[14]
Mitchel and Bennett have suggested that different supernumeraries have been associated with different effects on the adjacent dentition.[15] Foster and Taylor examined this relationship and found tuberculate types more commonly produced delayed eruption, whereas conical types produced displacement of adjacent teeth.[14] Eumorphic supernumeraries often erupt into the dental arch causing crowding.
A Supernumerary tooth should be removed if the above listed complications are identified. Extraction can be an immediate or delayed approach. Usually early surgical intervention is preferred which gives spontaneous eruption force to underlying permanent teeth and prevents extensive surgical / orthodontic treatment.[16] Possible disadvantage of early intervention is damage to adjacent teeth resulting in loss of vitality and root malformation. Before attempting surgical removal, the position of the supernumerary tooth must be localized and its relation to adjacent erupted and unerupted teeth and associated structures must be assessed. [17]
Several reports suggest that approximately 75% of unerupted permanent teeth erupt spontaneously in 2- 3 years, once the supernumerary tooth is removed. In cases where spontaneous eruption fails to occur, surgical exposure of the permanent tooth is indicated if there is sufficient arch space for eruption and lack of eruptive movement following removal of the supernumerary and after 6 month observation period. [1]
Case History:
A fourteen year old male reported to the Department of Pedodontics and Preventive dentistry, with a chief complaint of irregularity of lower front teeth. The family and medical histories were unremarkable.
Extra-oral examination did not reveal any abnormality. Intra-oral examination revealed a full set of permanent dentition, class I molar relationship and localized crowding in the upper and lower right anterior region.
Also noted was the presence of five incisors in the mandibular arch. Three mandibular incisors had erupted on the right side; with the most mesial one rotated almost 90° with lingual surface facing the midline. The other two mandibular incisors were in linguoversion. The mandibular right canine was buccally displaced. The maxillary right central incisor was inclined mesiolabially and the midline was shifted to the right. (Fig. 1, 2)
Intraoral periapical radiograph showed five mandibular incisors. The most mesial incisor on the right side, which was rotated, appeared to be slightly
 | Figure 1: Intraoral photograph of mandibular arch showing eumorphic supernumerary mandibular incisor indicated by the arrow.
 |
 | Figure 2: Intraoral photograph showing anterior crowding and eumorphic supernumerary mandibular incisor indicated by the arrow.
|
 | Figure 3: IOPA radiograph of the supernumerary tooth.
|
 | Figure 4: Orthopantomograph showing supernumerary tooth in the mandibular incisor region.
|
smaller in size. (Fig.3) This tooth was differentiated as eumorphic or supplemental supernumerary incisor.
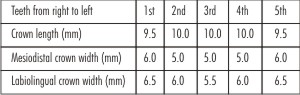 | Table - 1 Measurements of mandibular incisors.
|
OPG x-ray was taken which ruled out the presence of any other supernumerary tooth. (Fig.4). Tooth measurements obtained from study casts revealed that the dimensions of the eumorphic supernumerary incisor were similar to mandibular central incisor. (Fig.5),(Table 1). The eumorphic supernumerary tooth was extracted and orthodontic treatment was advised.
Discussion:
Prevalence of supernumerary teeth in the incisor mandibular region is about 1% of supernumerary prevalence and it is lowest in the oral cavity. [2] Extra teeth in the mandibular incisor region like other supernumerary teeth can be rudimentary or eumorphic in form.
Supplemental or eumorphic teeth as the name implies refers to duplication of teeth in the normal series. In the permanent dentition they appear most commonly as extra maxillary and mandibular lateral incisor, where as in the primary dentition they are most likely to appear as maxillary central incisors. [1]
The dichotomy theory of etiology proposes that a complete equal split of the tooth bud would result in two supplemental forms, whereas an unequal split would result in one normal tooth and one supernumerary tooth. Proponents of dental lamina theory believe that the supplemental form comes from the lingual extension of an accessory tooth bud, whereas the rudimentary form is derived from the proliferation of epithelial remnant of the dental lamina. [6]
A.Cassia et al reported a large Lebanese consanguineous family where four individuals displayed five incisors in the anterior mandible and suggested the involvement of single gene bearing recessive mutation. The identification of the gene by a whole genome screening will help to confirm this hypothesis and provide more information about pathogenesis.[18]
It may be difficult to distinguish the normal tooth from its supplemental "twin". A supplemental tooth may sometimes exhibit deep cingulum pit and have a coronal invagination.[1] In the present case, on the basis of measurements and position,
 | Figure 5: Maxillary and mandibular cast showing complete set of permanent dentition and supernumerary tooth in mandibular incisor region.
|
 | Figure 6: Extracted tooth specimen (labial view).
|
 | Figure 7: Extracted tooth specimen (mesial view).
|
 | Figure 8: Extracted tooth specimen (distal view).
|
 | Figure 9: Extracted tooth specimen (incisal view).
|
the supplemental supernumerary tooth resembled mandibular central incisor. However, morphologically it resembled more with the mandibular lateral incisor. The incisal edge was not at right angles to a line bisecting the crown labiolingually and the edge followed the curvature of the mandibular dental arch giving the crown the appearance of being twisted slightly on its root base (Fig.6-9). These are typical distinguishing features which differentiate a mandibular lateral incisor from a mandibular central incisor. [19].
Supplemental supernumerary teeth increase the crowding potential, causing an aesthetic problem, [1] inadequate plaque control and continued gingival inflammation. [20] These problems were also seen in the present case.
If both the teeth are equally well formed, the tooth that is displaced the most is to be extracted. [1] Therefore in this case we extracted the most displaced supplemental incisor. As moderate anterior crowding was present in both the arches, extraction of supplemental supernumerary tooth followed by orthodontic treatment should provide aesthetic results.
The frequency with which supernumerary teeth occur justifies complete initial radiographic examination because early detection is crucial if aesthetic and clinical complications are to be avoided or minimized.
References:
1. Hattab FN, Yassin OM, Rawashdeh MA. Supernumerary teeth: report of three cases and review of the literature. ASDC J Dent Child 1994; 61:382-93.
2. Rajab LD, Hamdan MAM. Supernumerary teeth: review of literature and a survey of 152 cases. Int J Pediatr Dent 2002; 12:244-54.
3. Babu V, Kikkeri SN, Diwakar NR. A rare case of hereditary multiple impacted normal and supernumerary teeth. J Clin Pediat Dentist 1998; 23:59-62.
4. King NM, Lee AMP, Wan PKC. Multiple supernumerary premolars: their occurrence in three patients. Aust Dent J 1993; 38: 11-16.
5. Mitchell L. Supernumerary teeth. Dent Update 1989; 16:65-9.
6. Primosch RE. Anterior supernumerary teeth: assessment and surgical intervention in children. Pediatr Dent 1981; 3:204-15.
7. Gravey MT, Barry HJ, Blake M. Supernumerary teeth: an overview of classification, diagnosis and management. J Can Den Assoc 1999; 65:612-16.
8. So LLY. Unusual supernumerary teeth. Angle Orthod1990; 60:289-92.
9. Luten JR. The prevalence of supernumerary teeth in primary and mixed dentitions. J Dent Child 1967; 34:346-353.
10. Tanaka S, Murakami Y, Fukami M. A rare case of bilateral supernumerary teeth in the mandibular incisors. Br Dent J 1998; 185(8):386-88.
11. Bodin I, Julin P, Thomson M. Frequency and distribution of supernumerary teeth among 21,609 patients. Dentomaxillofac Radiol. 1978; 7:15-17.
12. Locht S. Panoramic radiographic examination of 704 Danish children aged 9-10 years. Community Dent Oral Epidemol. 1980; 8:375-80.
13. Taylor GS. Characteristics of supernumerary teeth in the Primary and Permanent dentition. Dent Pract 1972; 22:203-8.
14. Foster TD, Taylor GS. Characteristics of supernumerary teeth in the upper incisor region. Dent Pract 1969; 20: 8-12.
15. Mitchel L, Bennet TG. Supernumerary teeth causing delayed eruption: a retrospective study. Br J Orthod.1992; 19:41-46.
16. Brin I, Zilberman Y, Azaz B. The Unerupted Maxillary central incisor-review of its etiology and treatment. J Dent Child 1982; 49:352-6.
17. Ibricevic H, Al-Mesad S, Mustagrudic D, Al-Zohejry N. Supernumerary teeth causing impaction of permanent maxillary incisors; consideration of treatment. J Clin Pediat Dentist 2003; 27:327-32.
18. Cassia A, El-Toum S, Feki A, Megarbane A. Five mandibular incisors: an autosomal recessive trait? Br Dent J. 2004; 197:307-9.
19. Ash MM, Nelson SJ. Wheeler's Dental anatomy, physiology and occlusion. The permanent mandibular incisors. 8th ed. St. Louis, Missouri: Saunders; 2007.p171-80.
20. Krayer JW. A suprrnumerry tooth located at the facial of a mandibular lateral incisor. J Periodontol.1989; 60: 410-12. |