Introduction
Trauma to the primary teeth may inflict injuries to various stages of developing permanent teeth. They may depend on the force with which injury is sustained to teeth related to age of the child resulting into cessation or at times failure to develop further leading to sequestrum formation. It also depends on the care and awareness shown by the patient's parents towards the treatment. An injury to the teeth of a young child can have serious and long term consequences.[1].
The position or shape of the tooth may be altered even before it erupts in the oral cavity and sometimes it may remain unerrupted [2].One of the reason for the noneruption of the teeth may be dilacerations. The term 'Dilaceration' refers to an angulation or a sharp bend or curve, in the root or crown of a formed tooth. The condition is thought to be due to trauma during the period in which the tooth is forming, with the result that the position of the tooth is formed at any angulation[3].Other authors have also described various cases in the literature.[4],[5] A typical case had been reported in the Department of Pedodontics.
Case Report
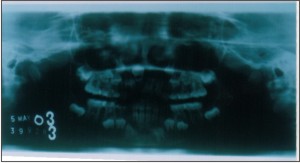
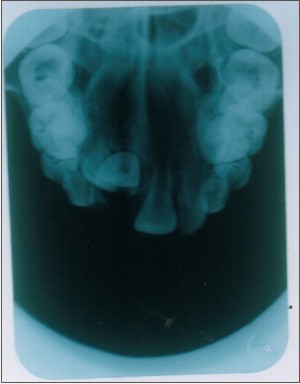
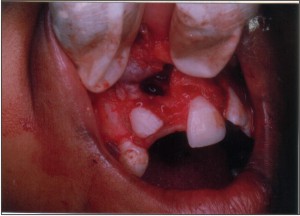
Nine year old female children reported to the dental clinic with the chief complain of Decayed teeth in the upper front region. The history of present illness included Decayed teeth since 1 year. No pain or swelling was present with to the decayed teeth and a missing tooth in the upper front region. The patient had undergone trauma in the front region of the face two years back. The mother revealed that the 51 had broken at the same time and the stump was left. Intraoral examination revealed Class I malocclusion with missing maxillary central incisor . No bulge was palpable in the maxillary vestibular area. An intraoral periapical radiograph was taken to ascertain the presence and position of the central incisor. The tooth was found to be impacted with dilaceration.
The other clinical findings were
Caries with 55, 54, 53, 63, 64, 75, 85, 84 and Grossly decayed 74, 61, 62, 74, 72, 52.
IOPA X-rays were advised with 74, 75, 84 and 85.
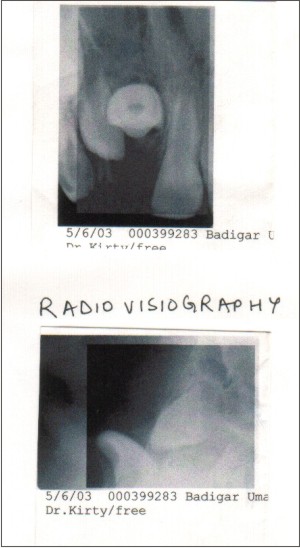
The Radiovisiographic view of 11 and 21 region was also done. The radiographic investigations revealed the presence of the unerupted and dilacerated central incisor below the nasal floor. The Radiovisiographic investigation helped in determining the exact position and angulation of the dilacerated tooth. The angulation and position (Inverted) of the tooth was such that the orthodontic extrusion was not possible hence it was decided to extract the tooth.
The routine Lab investigations like Hb, CT, BT, TLC, and DLC were also performed. The values were found to be in the normal range (HB-10.8gm%. TLC-8000cells/m3, DLC-P-50%)
The treatment phase started with the :
Oral prophylaxis
Topical fluoride application.
Restorations with 55, 54, 53, 63, 64, 75, 85, 84 followed by stainless steel crowns.
Extraction with 74, 61, 62, 74, 72, 52
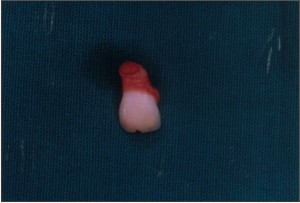
The surgical exposure with 11 region was carried out under local anesthesia. An incision was made and the buccal flap was raised. The Incisal edge of the tooth was slightly visible through a window in the labial cortical plate. Bone cutting was done to expose the crown completely followed by the extraction of the tooth .The curettage was done of the tooth follicle followed by copious irrigation .Sutures were placed to promote the healing.(Images 1-9)
The sutures were removed after one week and the healing of the area was uneventful. The patient is under regular supervision and regular recalls .A prosthesis with 11was planned later.
 | Image - 1
 |
 | Image - 2
|
 | Image - 3
|
 | Image - 4
|
 | Image - 5
|
 | Image - 6
|
 | Image - 7
|
 | Image - 8
|
 | Image - 9
|
Discussion and Review
A Dental surgeon who provides emergency care for a child after an injury to the primary teeth should be aware of the possibility of the damage to the underlying developing permanent teeth.
Intrusion injuries to primary teeth present the highest risk of damage to permanent tooth germs. Intrusion injuries are associated with damage to the pulpal and periodontal structures and possible fracture of the alveolar bone. The pulpal tissue of the intruded tooth sustains a severe shock during displacement, which may be reflected later by sequelae ranging from mild discoloration to pulpal necrosis and infection. Disintegration of pulpal tissue may result in periapical tissue inflammation, which in turn may induce developmental disturbances in the germ of the permanent successor tooth Many factors influence the sequelae of intrusion injuries: age, direction and severity of intrusion and type of treatment. Intrusive-type injuries to primary incisors most commonly take place between 1 and 3 years of age. Several reports have shown that the younger the child at the time of the intrusion injury, the more severe the induced sequelae to the successor tooth. [6], [7], [8]
Many studies have reported intrusive luxation to be the most frequent cause of developmental disturbances in permanent teeth. The intimate relation between the primary incisors and their successors explains the disruptive effect of intrusion injuries on permanent teeth. Children with a history of trauma experience a higher percentage of malpositioned incisors compared with those without trauma. This case presents a similar outcome, except that the severity of impact caused the successor to erupt with crown- root dilaceration.
Trauma to the deciduous teeth may have various implications such as enamel hypoplasias and dilacerations, the latter found to be far more common, with maxilla being more frequently involved than mandible. The prevalence of disturbances to the permanent teeth as a result of trauma to the primary teeth ranges from 13-57 percent. The likelihood of an injury affecting the development of the permanent tooth is dependent on the type and severity of the trauma, stage of permanent tooth development and the mode of treatment of the injury itself. [9], [10], [11]
Andreason and Ravn conducted a landmark clinical and radiographic study of 213 teeth, these investigators demonstrated that more than 40% of their young patients had changes in the permanent teeth could be traced to injury to the primary dentition. The close anatomic relationship between the apices of primary teeth and their developing permanent successors explains why injuries to primary teeth may involve the permanent dentition.
Developmental disturbances were classified into the following clinico-pathologic entities:
White or yellow-brown discoloration of enamel and horizontal enamel hypoplasia.
Crown dilacerations
Odontome - like malformation:
Root duplication:
Vestibular root angulation.
Lateral root angulations or dilacerations.
Partial or complete arrest of root formation
Sequestration of the entire tooth germ.
Permanent successors can be impacted (failure of eruption), delayed or accelerated in their eruption as a result of injuries sustained to deciduous teeth.
The premature loss of a deciduous tooth can either accelerate or delay the eruption of the permanent tooth depending on the stage of development of the succedaneous permanent tooth and the status of the surrounding bone [6], [7], [8], [9], [10], [11]
Kupietzky (2001) stated that the effect on the succedaneous tooth depends on the type of injury and age of its occurrence. The age of the child also determines whether damage to succedaneous teeth will result or not. The highest incidence of damage to the permanent tooth is between 0-2 years of age. The probability of a young child under 4 years of age having damage to permanent teeth after sustaining a traumatic injury is 60%.
Altun Ct (2009) presented the findings of a prospective 7-year study examining developmental disturbances of permanent teeth attributed to intrusive injury of their primary predecessors based on initial patient records and clinical observation A total of 78 children (aged 12-48 months) presenting with intrusive trauma to 138 primary incisors were available for follow-up examinations. The most frequently intruded primary teeth were maxillary incisors (93.47%), with the right central primary incisor representing 41.3% of all intruded teeth. In 23 patients, 36 teeth were scheduled for extraction during the first visit. During the course of follow-up, 41 of the remaining teeth exhibited post-traumatic consequences, including pulp necrosis (78.0%), internal and/or external root resorption (14.6%), ankylosis (4.9%), and obliteration of the pulp canal (2.5%). In 74 permanent successors (53.6%), >or=1 of the following developmental disturbances were observed: enamel hypoplasia (28.3%), crown and/or root deformation (16.7%), and ectopic eruption (16.7%).[12]
De Amorim Lde F(2011) conducted a study on One hundred forty-eight children (241 teeth) were followed up until the eruption of the permanent successor. The prevalence of developmental sequelae to permanent teeth was 22.4%. Discoloration and hypoplasia were the most frequent abnormalities (74.1%), followed by eruption disorders (25.9%). Age at the time of traumatic dental injuries to primary teeth was the only variable significantly associated with developmental sequelae to permanent teeth. Sequelae were most prevalent among children who suffered an injury between 1 and 3 years of age. They suggested that Children who sustain traumatic dental injuries should be followed up regularly for an early diagnosis and treatment of possible developmental sequelae to permanent teeth. [13]
In this case the brunt of the trauma to the primary teeth must have been so severe that the tooth follicle got inverted.
The actual mechanism of injury is usually the intrusion of the deciduous teeth. The prognosis of these teeth is not favourable; usually all the teeth remain unerupted.It is advisable to keep these patients under observation after trauma and to consult an orthodontist at an early stage in case of non eruption of the teeth. If the tooth remains unerupted, certain amount of space loss may occur.
References
1. Pediatric dentistry, Infancy through adolescence,3rd edition,J.R.Pinkham.W.B Saunders company.2001
2. Mourished F.A roentenographic study of dentigerous cysts. Incidence in population sample.Oral Surg Oral Med Oral Pathol 1964;18:47-53
3. Shafer WG,Maynard KH ,Bernet ML.Oral Pathology .W.B Saunders co: Philadelphia;1993 p-40
4. Van Gool AV.Injury to the permanent tooth germ after trauma to deciduous predessors.Oral Surg 1973;35:2-12
5. Smith JM.A Case of dilacerations.Dent Cosmos 1938;72;667
6. Andreason JO,Sundstrom B,Ravn JJ .The effects of the traumatic injuries to primary teeth on their permanent successors.A clinical and histological study of 117 injured permanent teeth.Scand J Dent Res 1971:79;219-83
7. Joshi MR.Dilaceration of all maxillary incisor crowns.JIDA 1964;36;39-40
8. Rodda JC. Gross maldevelopment of a permanent tooth caused by trauma to its deciduous predessors.N Z Dent J 1960:56:24-5
9. Taneja JR .Dilaceration of all maxillary incisors.JIDA 1966;38;8-9
10. Via WF Jr.Enamel defects induced by trauma during tooth formation.Oral surg Oral Med Oral Pathol:1968;25;49-54
11. Agnihotri A:Dilacerated unerrupted central incisor ;a case report.Journal of Indian Society of Pedodontics and Preventive dentistry .Sept 2006;24;3;152-154
12. Altun C, Cehreli ZC, Güven G, Acikel C. Traumatic intrusion of primary teeth and its effects on the permanent successors: a clinical follow-up study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Apr;107(4):493-8..
13. de Amorim Lde F, Estrela C, da Costa LR.Effects of traumatic dental injuries to primary teeth on permanent teeth--a clinical follow-up study. Dent Traumatol. 2011 Apr;27(2):117-21. |