Introduction:
Finger and partial-finger amputations occur as a result of traumatic injuries, congenital absences or malformations that present clinical challenges.[1] The loss of a finger produces significant functional deficiencies. In addition to immediate loss of grasp strength and security, finger absence may also cause marked psychological trauma. Although the intensity of this trauma varies among individuals, the psychological impact is not related to the magnitude of amputation.
Despite the advances in microsurgical techniques[2],[3],[4],[5],[6] the reconstruction of the amputated digits for a number of patients may not be successful and they can benefit more with passive prostheses.[7],[8] Moreover, access to surgeons who can perform digit re-plantation is minimal to nil for many patients in the developing countries.
Individuals who desire finger replacement usually have high expectations of the appearance of the prosthesis. The acceptance rate has been much higher when an individually sculpted custom restoration using silicone elastomer is provided.[9]
This paper aims to the prosthetic restoration of partial finger amputee along with additional retentive measures that can be prepared for prosthesis to ward off social stigmatization.
Case Report:
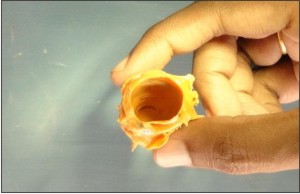
A female patient aged 18 years reported to department of Prosthodontics with a complaint of partial amputation of right middle finger (Fig 1). The amputation was made at the level of the intermediate phalanx. A finger prosthesis of silicone elastomer and acrylic nail was planned which could be retained mechanically by medical graded adhesive and additional ring with hooks, acrylic substructure with hooks & orthodontic transparent elastics.
Here, a methodology for fabrication of finger prosthesis is described that makes use of the patient's impression of the corresponding digit of contra lateral hand for making finger cast and wax pattern. Gypsum mould was made by investing finger wax pattern and was used for filling stained room temperature vulcanizing (RTV)-2 methyl silicone which was later left to cure at room temperature.
Steps for fabrication of finger prosthesis:
1. For digit (finger) impression Putty consistency of Vinyl poly siloxane was first kneaded and adapted well on corresponding digit of contra lateral hand and left for polymerization then the impression surface was scraped and vents were made for light consistency Vinyl poly siloxane to flow. Light consistency Vinyl poly siloxane later was injected on impression surface of putty finger
 | Figure 1 Partial amputation of right middle finger.
 |
 | Figure 2 Digit impression of corresponding digit of contra lateral hand.
|
impression and then placed back on the digit for polymerization, to get a fine detailed impression of digit (Fig 2).
2. Modeling wax was heated and then poured into the elastomeric finger impression, later it was left to cool to retrieve the finger wax pattern.
3. Similarly impression of partial finger amputee was also made and poured in dental stone to retrieve finger amputee cast. On this adjustable cast finger ring with hooks and acrylic substructure with hooks were prepared for additional retention.
4. On finger amputee cast an adjustable finger ring of nickel chromium was casted and hooks of orthodontic wire facing upwards were soldered on sides (Fig 3a).
5. For acrylic substructure with hooks approximately 0.5 mm to 1mm of finger cast was scraped at the tip to compensate compressibility of finger and plaster was built on top of finger amputee cast to create hollowness in prosthesis. Orthodontic wire was first adapted on tip of middle phalanx of finger amputee cast and hooks made of orthodontic wire facing downwards were soldered on sides was tried on patient to check the fit. Separating medium (sodium alginate) was applied on finger amputee cast on to which ring with soldered hooks were placed and by sprinkle on method 0.5mm thick acrylic ring (stained using acrylic stains) was prepared by self cure acrylic (Fig 3b).
6. Orthodontic elastic thread was tied on to hooks of cast finger ring and acrylic ring substructure to secure finger prosthesis in place and allow movement.
7. Carefully wax was scooped out from inside of wax pattern and was seated on finger amputee cast with acrylic substructure (Fig 4). Later the whole assembly (finger wax pattern with acrylic substructure) was tried on a partial amputee middle finger to check for fit.
8. Gypsum mould was made by investing finger wax pattern in a flask and by dewaxing after the gypsum sets.
9. Into this mould carefully stained RTV-2 methyl silicone using color corrected light was filled (Fig 5a), clamped and left to cure at room temperature (Fig 5b).
10. Deflasking was then done and finger prosthesis removed. Any excess flash on sides of prosthesis was cut using sharp scissors. Try in of finger
 | Figure 3 (a).Acrylic substructure with hooks reinforced with orthodontic wire;
|
 | Figure 3 (b) casted adjustable cast metal ring with soldered orthodontic wire hooks.
|
 | Figure 4 Finger wax pattern seated on finger amputee cast with acrylic substructure.
|
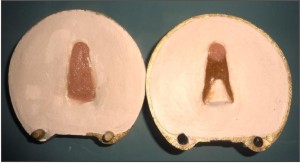 | Figure 5 (a).Stained RTV-2 methyl silicone filled into the gypsum mould: (b) flask being clamped and left to cure at room temperature.
|
 | Figure 6 (a). Try in of completed finger prosthesis with custom acrylic nail with nail paint (excess elastic thread was later cut );
|
 | Figure 6 (b) Finger prosthesis of patient in-situ.
|
prosthesis done (Fig 6a) and RTV- 1 methyl silicones was used to camouflage minor color discrepancies of completed finger prosthesis (Fig 6b).
11. Nail was made by staining clear acrylic using acrylic stains. Acrylic nail and acrylic substructure with hooks were attached to silicone finger prosthesis using cyanoacrylate glue.
Prosthesis so fabricated can be retained by using only medical grade adhesives & or by orthodontic elastic thread tied on to hooks of cast finger ring and acrylic ring substructure.
Discussion:
The elasticity, stability, and anti-staining properties of RTV-2 dimethyl polysiloxanes and their ability to replicate minute details make them widely popular for rehabilitation of amputee. They are often supplied in clear viscous liquids and thus can be easily pigmented to match the wide range of skin tones. Their curing process is initiated upon addition of the catalyst and therefore can be timed after the colour-matching process is completed, their slow curing rate allows sufficient time for the catalyzed mixture to be degassed to remove air bubbles prior, their curing rate can be hastened by oven-curing to meet tight work schedules and they can be made less viscous and pourable by the addition of silicone oil or organic solvents such as 111-trichloroethane and trichloroethylene.
RTV-1 methyl silicones are ready-for-use, self-curing silicones widely used in the industry as sealants, adhesives and coating agents. RTV-1 methyl silicones are useful when finishing prosthesis. The clear soft paste grades can be pre-mixed with color pigments and used to render subtle shades extrinsically on a completed prosthesis to camouflage minor color discrepancies.
The gentle, constant pressure of elastomer prosthesis can help desensitize and protect the injured tip.[10] The authors have noted that, over time, scar tissue contained within silicone prosthesis seems to become more pliant and comfortable. Similar observations have been reported in the medical literature although no conclusive proof has been established.[11],[12],[13] Recent literature speculates that silicone gel improves the hydration of the stratum corneum of immature hypertrophic scars.[14]
Finger prosthesis should be biocompatible, strong, and stable. In addition, the material should be skin like in color and texture. Characteristics such as a pleasing shape, thin margins, lifelike fingernails, and realistic color, contours and detail are also essential for patient satisfaction. This level of restoration is most successful when finger prostheses are individually sculpted and colored in situ under a variety of lighting conditions.
The fit of the prosthesis on the stump is another important concern of the patients: a tight fit causes discomfort while a loose fit can cause embarrassment if the prosthesis falls off in public. Pereira et al[15] reported that about a quarter of their 90 patients experienced the poor or loose fit of their finger prosthesis.
Finger prosthesis delivered to the patient was made more strong and stable by using acrylic substructure. For additional retention orthodontic elastic thread was tied on to hooks of cast finger ring and acrylic ring substructure to secure finger prosthesis in place and allow movements. Orthodontic elastic thread of 0.25 used to hold the finger prosthesis by tying on to hooks of cast finger ring and acrylic ring substructure are used routinely to secure or hold arch wires in the brackets and also can be used to apply force. Like rubber, however, these elastomers tend to deteriorate in elastic performance after a relatively short period. This feature does not prevent them from performing quite well and can be changed at an interval of 2 weeks. The preformed rectangular orthodontic archwires often listed in the catalogs as "arch blanks" and the name is appropriate, since this properly implies that a degree of individualization of the shape of the preformed arch wires will be required to accommodate the needs of patients.[16] This holds good for the orthodontic arch wire 0.019 X 0.025 SS used in this case report as it accommodates the needs of the patient by providing strength as well as esthetics (as it is only 0.019 X 0.025 well hidden in acrylic substructure) to the finger prosthesis.
Conclusion:
The loss of even one finger produces significant deficiencies. Apart from the psychological trauma a dexterous individuals suffer the greatest degree of impairment. Finger prosthesis with orthodontic elastic tied on to hooks of cast finger ring and acrylic ring substructure for additional retention can often restore near normal function in distal phalange amputations.
References:
1. Beasley RJ. General considerations in managing upper-limb amputations. Orthop Clinics of North Amer 1981;12 (4):743-749.
2. Bickel KD, Dosanjh A. Fingertip reconstruction. Journal of Hand Surgery. 2008;33: 1417-1419.
3. Hattori Y, Doi K, Sakamoto S, Yamasaki H, Wahegaonkar A, et al. Fingertip replantation. Journal of Hand Surgery 2007; 32: 548-555.
4. Shi D, Qi J, Li D, Zhu L, Jin W, et al. Fingertip replantation at or beyond the nail base in children. Microsurgery 2010;30: 380-385.
5. Beris AE, Lykissas MG, Korompilias AV, Mitsionis GI, Vekris MD, et al. Digit and hand replantation. Archives of Orthopaedic and Trauma Surgery 2010;130: 1141-1147.
6. Molski M. Replantation of fingers and hands after avulsion and crush injuries. Journal of Plastic, Reconstructive and Aesthetic Surgery. 2007; 60: 748-754.
7. Alison A, Mackinnon SE . Evaluation of digital prostheses. Journal of Hand Surgery 1992;17: 923-926.
8. Livingstone DP. The D-Z stump protector. Amer J Occu Ther 1988;42:185-187.
9. Buckner H. Cosmetic hand prostheses- a case report. Orthotics and Prosthetics 1980;34 (3):41-45.
10. Ohmori S. Effectiveness of silastic sheet coverage in the treatment of scar kebid. Plas Surg 1988;12:95-99.
11. Quinn KJ. Silicone gel in scar treatment. Burns 1987;13:533-540.
12. Wessling N, Ehleben CM, Chapman V, et al. Evidence that use of a silicone sheet increases range-of-motion over burn wound contractures. J Burn Care and Rehab 1985;6:503-505.
13. Burkhardt A, Weitz J. Oncologic applications for silicone gel sheets in soft-tissue contractures. Amer J Occu Ther 1990;45(5):460-462.
14. Wilson RL, Carter Wilson MS. Rehabilitation after amputations in the hand. Orthopedic Clinics of North America. 1983;14: 851-872.
15. Pereira BP, Kour AK, Leow EL, Pho RWH. Benefits and use of digital prostheses. Journal of Hand Surgery. 1996; 21: 222-228.
16. Contemporary Orthodontics.William R. Proffit, Henry W. Fields & David M. Sarver. St. Louis: Elsevier Inc.; 2009.p.372 and 428. |