Introduction
The severely atrophic ridges pose a clinical challenge for the fabrication of a successful complete denture because of decreased supporting tissue and denture bearing area. Also as the ridge resorption progresses, the resultant large inter-ridge space leads to fabrication of heavy complete dentures which adds to decrease in retention and stability of the denture.
Reducing the weight of the prosthesis may help in improving its retention and this may be achieved by making hollow dentures. Historically, weight reduction approaches have been achieved using a solid 3-Dimensional spacer including dental stone [1],[2],[3],[4],[5],[6],[7] cellophane wrapped asbestos[3], silicone putty[2],[3],[4],[5], [6] or modeling clay[4] during laboratory processing to exclude the denture base material forming a hollow cavity in the prosthesis.
This clinical report describes a technique in which a hollow maxillary complete denture was fabricated using silicone putty as a solid spacer.
Clinical Report
A 72-year-old male patient reported to the department of Prosthodontics, with a chief complaint of fractured upper denture and desired the replacement of the same(Fig. 1). On taking the history, patient reported that maxillary complete denture is quite bulky and he is unsatisfied with the same because of its weight.
The medical history of the patient revealed hypertension since last 10 years and the patient was on medication for the same. The duration of edentulousness was 2 years and teeth were lost due to periodontal reasons and ever since patient was a denture wearer.
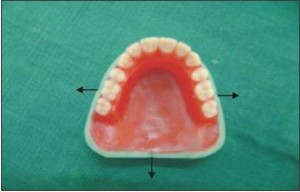
On clinical examination completely edentulous upper and lower ridges with severe atrophy of maxillary residual ridge was noticed (Fig. 2). Mucosa of the patient was healthy, firm and resilient. On examination of the old denture, the maxillary complete denture was found to be quite bulky in nature.
This clinical report describes a technique for fabrication of hollow maxillary denture that was selected as a treatment modality for the patient.
Technique
Primary and secondary impressions of maxillary and mandibular residual ridges were made using
 | Figure 1 Extraoral Pre-operative View Of The Patient.
 |
 | Figure 2 Intraoral Pre-operative View Of The Patient Showing Severe Atrophy Of Maxillary Residual Ridge.
|
 | Figure 3 Indexing The Land Area Of The Maxillary Master Cast For Reorientation Of Clear Template.
|
 | Figure 4 Flask Showing Waxed-up Cast For Second Denture Base And
|
 | Figure 5 Duplicated Cast Used To Fabricate Clear Template Using 1mm Thick Thermoplastic Sheet.
|
 | Figure 6 Duplicated Cast Used To Fabricate Clear Template Using 1mm Thick Thermoplastic Sheet.
|
conventional techniques. Jaw relations were recorded and the teeth arrangement was completed. Trial was done with patient's satisfaction.The land area of the maxillary master cast was indexed using a triangular file and trial denture base was sealed to the definitive cast using base plate wax (Fig. 3). This waxed up trial denture was duplicated using irreversible hydrocolloid (Plastalgin alginate) and poured in dental stone (Gypstone type III, Dentpro Pvt. Ltd.). (Fig. 4)
The duplicated cast was used to make a clear template, using 1mm thick thermoplastic sheet (Polypropylene sheet, Bioplast) (Fig 5). Two flasks with interchangeable bases were selected. The maxillary trial denture base was flasked using 3 pour technique and processed by a conventional method till wax elimination stage.
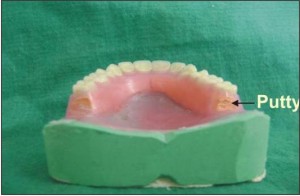
The base of the flask having the master cast was separated and cast was again waxed up for making the permanent denture base using a second flask.(Fig 6). The permanent denture base was made with heat cure polymerized resin (DPI, Heat cure, Mumbai, India) and the clear template which was made earlier was placed on the cast using indices in the land area as seating guides. An endodontic instrument with a rubber stop was used to measure space between the clear matrix and permanent denture base (Fig. 7). Horse shoe shaped silicone putty (3 M ESPE A.G Dental products, Seefeld, Germany) was mixed and adapted to the permanent denture base(Fig 8) leaving about 2-3 mm of space between the putty and the clear matrix and an additional space of 1 mm over the tooth portion of the denture. (Fig 9).After verifying the adequate space, the clear matrix was removed and putty was fixed to the roughened permanent denture base using tray adhesive (3 M ESPE A.G Dental Products Seefeld Germany). The base with master cast having permanent denture base and putty over it as spacer was packed along with the first flask in which teeth were left after dewaxing, using heat cure polymerized resin (DPI heat cure, Mumbai, India) and curing was carried out.
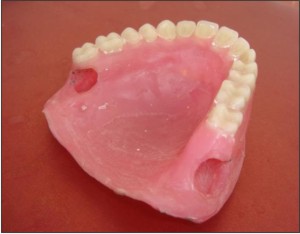
After conventional processing procedures, the denture was retrieved and putty was removed using a sharp scraping instrument, forming a cavity (Fig. 10 & 11). Two covers using self cure polymerizing resin (DPI RR cold cure, Mumbai, India) were made and windows of the cavity in the denture were sealed with them. The denture was polished in a usual manner. The denture was immersed in
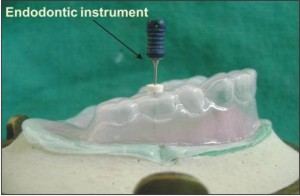 | Figure 7 An Endodontic Instrument Used To Measure Space For Putty Spacer Between Clear Template And Permanent Denture Base.
|
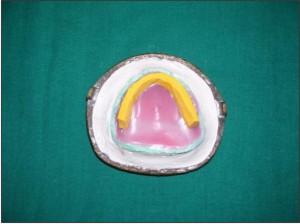 | Figure 8 The Flask Having Maxillary Master Cast With Permanent Denture Base And Putty Over It.
|
 | Figure 9 Clear Template Over The Putty Spacer.
|
 | Figure 10 Denture Retrived After Deflasking
|
 | Figure 11 Putty Spacer Removed From The Cavity With Sharp Scraping Instrument.
|
 | Figure 12 Hollow Floating Denture.
|
 | Figure 13 Intraoral Post Operative View Of The Patient With Dentures In Place.
|
 | Figure 14 Extraoral Post Operative View Of The Patient.
|
water to check for any seepage of water into the cavity.(Fig. 12). During insertion of complete denture it was checked for border extensions, proper adaptation and occlusion.(Fig 13,14).Patient was recalled after 24 hrs. to correct any sore spot and occlusal discrepancy and again recalled after 48 hrs,1 week, 3 week, 6 week and then after 3 months to correct the problem associated with wearing of denture. The patient reported with improved retention of maxillary complete denture and reduced bulkiness of the denture.
Discussion Extreme resorption of the ridge whether maxilla or mandible will lead to a reduced denture bearing area which in turn will affect retention, stability and support for the complete denture. Problems that are likely to be faced may be due to narrower and more constricted residual ridge as the resorption progresses, causing reduced supporting tissue with larger restorative space between maxillary and mandibular residual ridges. Extensive volume of the denture base material in prosthesis provided to patients with large maxillofacial defects or severe residual ridge resorption is always a challenge to prosthodontists .To increase the retention and stability of heavy prosthesis, many methods have been tried like utilizing the undercuts, modifying the impression technique, use of magnets , use of implants , etc. Apart from this, when we look into the history of bulkier prosthesis reduction in prosthesis weight also have been tried by making the denture hollow. Such weight reduction approaches have been achieved using a solid 3-dimensional spacer including dental stone, cellophane wrapped asbestos, silicone putty or modelling clay during the laboratory procedures which are removed later to provide a hollow denture base.
The advantages of hollow dentures are reduction in the excessive weight of the acrylic resin, resulting in the lighter prosthesis, decreases the load on the residual alveolar ridge making the patient comfortable. The method described in the paper for fabrication of hollow denture has advantages over previously described methods for making hollow denture[3],[4]. Leakage and difficulty in measuring the resin thickness were the problems associated with other techniques[8]. Heat polymerizing one portion of the denture against polymerized resin may reduce leakage at the junction of the two portions of the denture. The use of a clear pressure formed matrix of trial denture facilitates the fabrication of silicon putty cavity form.
Use of silicone putty has advantages of its stability, ability to be carved and that it does not adhere to acrylic resin. It can be stabilized by use of tray adhesive that can be easily separated later. This technique ensured the uniform thickness of acrylic resin by visualizing space between putty and clear template and to measure it with a sharp endodontic instrument that can easily penetrate the clear template. This technique resulted in marked reduction in weight of complete denture from 20.6 gm (Old maxillary complete denture) to 11.65 gm (Newer maxillary complete denture). This lead to decrease in the bulkiness of the denture. (Fig. 9).
Summary & Conclusion
Rehabilitation of severely resorbed ridges is a challenge to the prosthodontist. Even though, the choice of rehabilitation can be overdentures, implant retained over-dentures, ridge augmentation, etc, many a times the patients who comes with such a problem are geriatric patients with many systemic illness. Hence, the best way is to rehabilitate them with conventional complete dentures. Apart ,from modifying the impression technique to get maximum denture bearing area, modifying the type of denture also may be better accepted by patients. Hence, loose denture weight for healthy and comfortable living.
References
1. EL Mahdy AS. Processing a hollow obturator, J Prosthet Dent 1969; 22: 682-6
2. Holt RA Jr. A hollow complete lower denture. J Prosthet Dent 1981; 45: 452-4.
3. Worley JL, Kniejski ME, A method for controlling the thickness of hollow obturator prosthesis J. Prosthet Dent 1983; 50: 227-9.
4. Elliott DJ. The hollow bulb obturator: it fabrication using one denture flask Quintessence Dental Technol 1983; 7: 13-14.
5. Fattore LD, Fine L Edemonds DC, The hollow denture; an alternative treatment for atrophic maxillae. J Prosthet Dent 1988; 59: 514-6.
6. Jhanji A, Stevens ST Fabrication of one -piece hollow obturators. J Prosthet Dent 1991; 66: 136-8.
7. McAndrew KS, Rothenbergers An innovative investment method for the fabrication of a closed hollow obturator prosthesis. J Prosthet Dent 1998; 80: 129-150.
8. Sullivan and Hansen. The hollow maxillary complete denture. A modified technique, J Prosthet Dent 2004; 91: 591-4. |