Introduction:
Impaction is defined as the total or partial lack of eruption of a tooth well after the normal age for eruption. An impacted tooth may appear blocked by another tooth, bone, or soft tissue, but the cause of tooth impaction is often unknown[1].
Orthodontic movement of the impacted tooth after surgical exposure is the most common treatment (except for third molars). Bringing an impacted or unerupted tooth into the arch creates a set of special problems during alignment. The problems in dealing with the unerupted tooth fall into three categories, surgical exposure, attachment to the tooth, orthodontic mechanics to bring the tooth into the arch[2].
This article describes a case of an impacted maxillary central incisor which was brought into the arch using simple orthodontic procedures.
Case Report:
A 12yr old female patient reported for orthodontic treatment with a chief complaint of missing upper front tooth. The general health of the patient was good with no significant medical history. A clinical oral and dental examination revealed an Angle Class II subdiv malocclusion with moderate crowding in the lower arch. The maxillary left central incisor was absent in the oral cavity, and the upper midline was deviated to the left while the lower midline was coincident with the facial midline. (Fig.1-2)
Radiographic Examination:
On examination of the OPG, IOPAs & Lateral cephalogram, it was concluded
 | Fig 1 Pre treatment frontal smile photograph
 |
that the left central incisor was bucally impacted and there was insufficient space for the central incisor to erupt. (Fig.3)
Diagnosis:
A 12 years old female patient, having Class I skeletal relation, impacted left central incisor, end on molar and canine relation on right and class I on the left side, deep bite and poor smile esthetics.
Treatment Plan:
Analyzing the clinical and radiographic findings, it was planned to first level and align the upper and lower teeth. This will be followed by creation of sufficient space for the impacted maxillary central incisor while correcting the midline. On gaining sufficient space for the incisor, it will be exposed surgically, bonded and moved into the arch. The use of overlay archwire was decided for traction of impacted tooth because of its various advantages described below. After the alignment of arches, other orthodontic objectives like opening of bite, correction of molar and canine relation were to be achieved.
Treatment Progress:
The first molars were banded and all maxillary and mandibular teeth were bonded using 0.022" slot brackets. After initial leveling and aligning of the arches (Fig 4), space was created for the impacted central incisor with the help of an open coil spring. The impacted central incisor was exposed by an apically repositioned flap. A curved base attachment (Begg bracket) was bonded on to the central incisor and a ligature wire was tied to it. The raised flap was sutured back and the ligature was tightly tied to the main arch wire of the upper arch (Fig.5). In order to bring the central incisor in the arch a overlay ('piggy back') wire of 0.014" NiTi, over a 0.019"x0.025" stainless steel wire, was engaged on the begg bracket of the central incisor[2] (Fig.6). The overlay wire extended from second premolar on right side to the second premolar on the left
 | Fig 2 pretreatment intraoral photographs
|
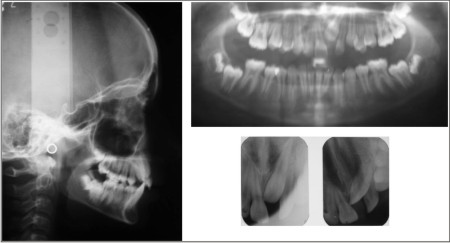 | Fig 3 pretreatment radiographs
|
 | Fig 4 initial leveling and alignment
|
 | Fig 5 surgical exposure and bonding of attachment on impacted incisor after creation of adequate space
|
side. Once enough of the crown of the impacted tooth appeared, a suitable bracket was bonded to it for further leveling and alignment and continous 0.014" NiTi was inserted (Fig 7), followed by 0.019"x0.025" NiTi and finally 0.019"x0.025" stainless steel wire. Bracket repositioning was done to correct the root position.
Treatment Results:
The impacted central incisor was successfully brought into the line of arch. All the orthodontic treatment objectives were achieved.
The patient's smile esthetics improved considerably (Fig.8-10). The gingival zenith of the left central incisor was higher than that of the right. Because the patient had a low smile line, however that discrepancy was not evident on smiling.
Discussion:
Although the ideal treatment for impactions is preventive, a number of
 | Fig 6 overlay archwire for traction of impacted canine
|
 | Fig 7 bonding of bracket on central incisor and final alignment of arch
|
 | Fig 8 Post treatment frontal smile photograph
|
 | Fig 9 Post treatment Intra Oral Photographs
|
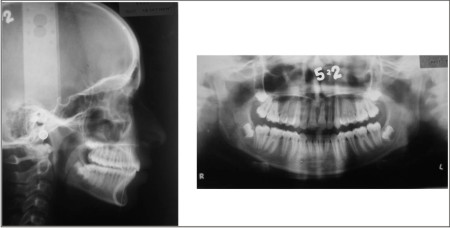 | Fig 10 Post treatment radiographs
|
surgical and orthodontic techniques are available for aligning impacted teeth when necessary. Currently, the most common procedure is bonding of an attachment directly to the enamel surface of the impacted tooth at the time of surgery. This technique requires a minimum amount of bone removal to expose the portion of the crown to be bonded. Tooth can be brought into the arch using a variety of traction methods like use of elastomeric chains, lasso wire, removable appliances or various types of springs. These traction methods have various disadvantages. A wire lasso around the cemento-enamel junction of the tooth has been found to damage the tooth and periodontal tissue.[3] Elastomeric chain exerts a high initial force that deteriorates rapidly, and it also tends to accumulate plaque, which makes it unsuitable for use under a flap. Wire systems are rigid and can be uncomfortable if the traction is not applied along the entire length of wire[4]. Wire fatigue can lead to fracture or difficulty of ligation to the traction archwire.
Superelastic wires like NiTi wires, with shape memory and ability to exert a light, continuous force over a considerable distance can be used for applying orthodontic traction to impacted teeth [5], [6]. A NiTi wire overlay on a rigid main archwire can effectively bring an impacted tooth into the arch while maintaining the anchorage and archform. Activation is also simple and does not depend on patient cooperation, as with removable appliances or elastics. Another benefit of using overlay archwire is that the tooth erupts in the line of the arch, through keratinized mucosa, which increases the likelihood of long-term periodontal health[7]. One drawback of this system is that if the bracket comes off during traction, another surgery is required to replace it.
Conclusion:
The overlay wires are an effective alternative to various traction methods used for bringing impacted teeth into the line of arch. They apply very gentle and light force during alignment and help in bringing the tooth very close to the line of arch while maintaining its periodontal health, the archform and anchorage.
References:
1. Glossary of dentofacial orthopedic terms (orthodontic glossary). St Louis: American Association of Orthodontics, 1993.
2. Proffit WR, Fields HW, Sarver DM: Contemporary Orthodontics, Fourth edition,564,2007
3. Boyd, R.L.: Clinical assessment of injuries in orthodontic movement of impacted teeth, Part I: Methods of attachment, Am. J. Orthod. 82:478-486, 1982
4. Oliver, R.G. and Hardy, P.: Practical and theoretical aspects of a method of orthodontic traction to unerupted teeth illustrated by three cases, Br. J. Orthod. 13:229-236, 1986.
5. Samuels RHA, Rudge SJ.: Two-Archwire Technique for Alignment of Impacted Teeth J Cli.Orthod.31:183-187,1997
6. Miura, F.; Mogi, M.; Ohura, Y.; and Hamanaka, H.: The super-elastic property of the Japanese NiTi alloy wire for use in orthodontics, Am. J. Orthod. 90:1-10, 1986
7. Kokich, V.G. and Mathews, E.P.: Surgical and orthodontic management of impacted teeth, Dent. Clin. N. Am. 37:181-204, 1993 |