Introduction
In order to provide a high quality orthodontic care to our patients , it is essential to know the cause of malocclusion. Ranly[1] proposed a composite view , stating that the chondrocranium is influenced by both intrinsic, genetic and local environmental factors.
Altered mode of breathing through mouth is an adaptation to obstruction in nasal passages . The obstruction may be temporary and recurrent while more often it is partial than complete , the airway resistance enough to force the subject breathe through mouth . Studies in human subjects also have shown that airway obstruction causes alterations in craniofacial development . It has been observe by most Pediatrician in kanpurites population that allergic rhinitis(chronic) is the most common cause of mouth breathing . The purpose of this study was to compare the dental and facial skeletal characteristics of children afflicted with allergic rhinitis who were apparent mouth breathers , their siblings who did not have the disease and were apparent nose breathers. Harvolds[2],[3] classical study on artificially nasally obstructed monkey suggested that neuromuscular changes required to maintain an open oralairway contributed to the skeletal and dental changes . Solow[6] and Kreiborg put forward the soft tissue stretch theory in which they suggested that the obstruction to the airway is a major causative factor in determining the facial morphology.
Material and Method
Twenty pair were evaluated: allergic children and their non-allergic siblings .Subjects include kanpurite population of either sex with an age range of 8-14 (Tab1) years. Mean age difference between siblings was one year nine months (Tab2). Concent of parents and patients is taken before the study was performed.
Selection Criterion for allergic children
1) History of chronic mouth breathing as perceived by the parents.
2) History of chronic nasal congestion.
3) Allergic rhinitis as confirmed by pediatrician.
4) No history of septal deviation, orthodontic treatment or facial trauma.
5) No history of pacifier use are digit sucking past five year of age.
Selection Criterion for non-allergic siblings
1) Nasal breathing as perceived by the parents.
2) No history of chroic nasal congestion.
3) No history of allergic rhinitis.
4) No history of septal deviation, orthodontic treatment or facial trauma.
5) No history of pacifier use or digit sucking habit beyond 5 years of age.
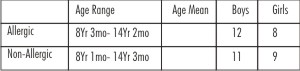 | Table1:-Distribution of subjects by age and sex
 |
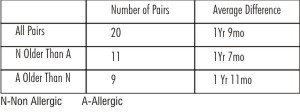 | Table2:-Age difference between siblings
|
Medical Examination
Every subject was examined by pediatrician to rule out anatomic abnormalities an amount of mucosal edema. Nasal smears were then analysed to determine the percentage of eosinophils in the mucous.
Orthodontic Examination
Intra oral:- Following informations to be observed
Teeth present, maxilla and mandibular dental midlines incentric relation and centric occlusion,
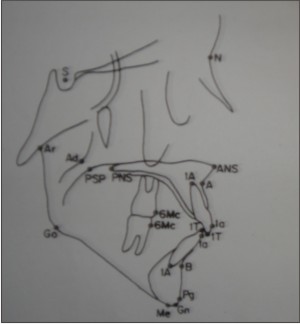 | Fig 1 Dental And Skeletal Landmarks
|
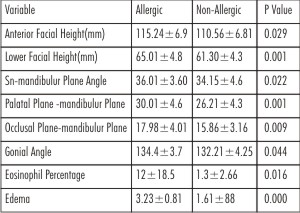 | Table 3 Variables That Were Significantly Different Between The Sibling Pairs
|
 | Table 4 Comparison Of The Means For Selected Variables Among The Groups
|
presence of centric relation to centric occlusion shifts, right and left first molar and canine relationships, transverse malrelationships, presence of open bite, maxillary and mandibular intermolar and intercanine widths.
Cephalometric Analysis:- Cephalometric radiographs for all subjects were taken by standard method prescribed by broandbent. The radiographs were taken with the subjects teeth in centric occlusion and their lip at rest. Tracing of the radiographs were made on 0.003 inch matte acetate paper with a 0.3mm pencil. Twenty four dental and skeletal landmarks(Fig-1) were identified to produce following linear and angular measures.
Angular:- SNA, SNB, ANB, SN-Pg, SN to Pallatel plane, SN to occlusal Plane, SN to mandubulur plane, ramus angle, SN to upper 1 axis, lower 1 axis to mandibular plane interincisal angle, palatal to mandibular plane, occlsal palne to mandibular plane, gonial angle.
Linear:- Total anterior facial height, posterior facial height mandibular length, upper 1- NA, lower 1 - NB, overjet, overbite.
Statistical Analysis:- Dependent t tests were performed to determine the differences between the sibling pairs, multiple regressions were performed to determine whether allergies had a significant effect on the dependent variables. Statistical significance was defined as P<0.05.
Error Analysis:-Six randomly selected films were retraced and measured to determine intrarater reliability. A high degree of reliability was found.
Results
Comparison Between Sibling Pairs
Medical examination & history The amount of edema present in the nasal mucosa and the percentaze of eosinophils in the nasal smear were both significantly greater in the allergic siblings.
Dental relationships Allergic children shows significantly larger palatal height, their is no significant difference between group for maxillary and mandibular intermolar and intercanine width. Incidence or degree of anterior dental open bite is slightly more in allergic children. Angle of mandibular permanent incisor to the mandibular plane was significantly smaller in the allergic group.
Skeletal Relationships (Tab3) Allergic siblings shows increase in total anterior facial height and lower facial height. The gonial angle and the angular measures of mandibular plane to SN , palatal plane .and occlusal plane were all significantly greater in the allergic children .The allergic subjects demonstrated a tendency toward retrognathia with the SNA SNB and SN-pogonion angles being slightly smaller, though not significantly different,than in the nonallergic group .The ANB angle was approximately equal for both groups .
Comparison Of Group Means Among Allergic And Nonallergic Subjects (Tab 4)
There were several significant skeletal and dental differences between the allergic group and the nonallergic sibling. The palatal height was larger in the allergic group ,demonstrating tendency for increased vertical dimensions .The amount of overjet in the allergic subjects was also larger ,the mandibular incisor to mandibular plane angle was decreased.
Discussion
The study was conducted to evaluate the relationship between facial growth and nasal obstruction caused by allergic rhinitis .Earlier it was found that obstruction of nasal passage leads to a change in respiration and can influenced the pattern of facial development .Others have refuted the theory that an altered mode of breathing affects facial development Some claiming that growth is determined primarily by genetic factors . Siblings pairs were used in this study in an attempt to differentiate the facial characteristics most strongly determined by heredity from facial structures more vulnerable to environmental influences specifically mode of breathing .
Facially the most striking difference found between the siblings pairs were evident in vertical plane ,with the allergic children expressing a more divergent facial pattern .Hannuksela[8] in a study of 100 11yr old subjects grouped according to size of adenoids and degree of atopy , also found increases in the vertical plane in moderate and severely atopic children Overall she reported that with increasing severity of allergy and increased adenoid size ,there was a dorsal rotation of the mandible . In Sassouni and associates study of the difference between allergic rhinitis ,their siblings ,and controls they reported that 37 children with allergic rhinitis had a longer and narrower facial structure. Bresolin[7] and associates who also studied allergic rhinitis children as compared with controls ,confirmed these results ,demonstrating an elongated and more retrognathic skeletal type in the allergic children .
In this study the difference between anterio posterior and vertical measures suggest that the effects of allergic rhinitis are expressed primarily in vertical plane,whereas the anterio posterior relationships are governed primarily by genetic factors .In a study compairing sibling pairs and controls ,Sassouni[9] and associates also found this trend .The results of this study support theory that in a child with genetic predisposition to a long face an alteration in breathing mode resulting from an allergy can increase the expression of the long face tendency.
Conclusion
From the above study it was concluded that there is a critical time during growth when changes associated with nasal allergy become irreversible .Controlled longitudinal studies evaluating cause and effect dependence and the value of medical and surgical intervention should be undertaken .It was also concluded that the developing malocclusion should be intercepted and treated accordingly
References
1. Ranly DM. Theories of craniofacial growth. In Ranly DM ,ed A synopsis of craniofacial growth. New York; Appleton-Century Crofts, 1980.
2. Harvold EP ,Vargervik K, Chierici G . Primate Experiments on oral sensation and dental malocclusions . Am J Orthod 1973; 63: 494-508.
3. Harvold ,Vargervik K,Chierici G . Primate experiments on oral respiration .Am J Orthod 1981;79:359-72 .
4. Linder-Aronson S . Effects of adenoidectomy on dentition and nasopharyx . AM J ORTHOD 1974 ;65:1-15 .
5. Dunn G F, Green LJ, Cunat JJ Relationship between variation of mandibular morphology and variation of nasopharyngeal airway size in monozygotic twins .Angle Orthod 1973;43:129-35 .
6. Solow B ,Kreiborg S . Soft tissue stretching a possible control factor in craniofacial morphogenesis . Scand J Dent Res .1917; 85: 505-07
7. Bresolin D, Shapiro PA , Shapiro GG, Chapko MK, Dassel S Mouth breathing in children: Its relationship to dentofacial development .Am J ORTHOD 1983; 83:334-40 .
8. Hannuksela A The effect of moderate and severe atopy in facial skeleton . Eur J Orthod 1981 ;3:187-93 .
9. Sassouni v, Friday GA ,Shnorhokion H , Beery Q ,Zullo TG, Miller Dl ,Murphy SM , Landy RA . The influence of perennial allergic rhinitis on facial type and a pilot study of the effect of allergy management on facial growth pattern . Ann Allergy 1985;54: . 493-7
10. Quick LA. Gundluch KH. Adenoid facies. Laryngoscope 1978:88:327:33/
11. Watson RM. Warren DW Fisher ND Nasal resistance skeletal classification and mouth breathing in orthodontic patients. AM J Orthod 1958:54:367:79.
12. Orgaard B Larsson E Lindsten R. The effect of sucking habits, cohort, sex, intercanine arch widths, and breast are bottle feeding on posterior crossbite in Norwegian and Swedish 3 years old children. AM J.orthot dentofac Orthop 1994:106:161-66
13. Cheng MC etal. Developmental effects of impaired breathing in the face Of the growing child. Angle orthod 1988:58:309-20.
14. Kerr WJ,Mc William JB Linder- Aronson S.Mandibular forma and position related to changed mode of breathing-a 5 year longitudinal study.Angle Orthod 1989:59:91-96 |