Introduction
The study of tooth movement begins with an understanding of cellular and molecular mechanisms that enable the periodontal tissues to adapt to orthodontic forces.This was considered a challenging task due to the inaccessibility of bone and its surrounding tissues in human subjects undergoing orthodontic treatment. Experimental studies on animal models have been used to understand the tissue response to orthodontic forces.But the conclusions based on these studies have to be viewed with caution as species differ in basic morphology, growth pattern, turnover rate and tissue reaction. A better understanding of the specific biochemical pathways in individual patients provides the key to prediction of the specific response to mechanical forces.Gingival crevicular fluid (GCF) has emerged as a useful, non-invasive method for assessing tissue responses. The study of its composition helps to understand the histological response to orthodontic forces in our patients. The intra-cytoplasmic enzyme Aspartate aminotransferase (AST) is released into the extra-cellular environment upon cell death.The monitoring of AST activity in GCF reflects the magnitude of periodontal tissue destruction. Therefore, the present study was designed to estimate the levels of enzyme AST in GCF during orthodontic tooth movement.
Review Of Literature
Karmen et al (1955)[1] studied the transaminase enzymes (Glutamic-oxaloacetic transaminase & Glutamic-pyruvic transaminase) in the human blood. They demonstrated the transaminase activity in human serum & blood cellular elements as well as variation in enzymatic activity in the blood of normal & diseased man.
Reitan (1957)[2] performed a series of human experiments and measured the force applied and the distance through which the teeth were moved. He concluded that orthodontic forces produced hyalinised areas on the pressure side of the tooth moved.
Lilja, Lindskog, and Hamm (1983)[3] studied orthodontic tooth movement in rats using histochemical techniques for enzymes associated with bone resorption and tissue damage. They moved maxillary first molar buccally by means of a fixed appliance with predetermined forces for periods of from 10 hours to 6 days. Their results showed that the activities of acid phosphatase and lactate dehydrogenase were higher in cells in the connective tissue of the periodontal membrane (PDM) than in the oral mucosa.
Chambers et al (1991)[4] showed enzymatic increase of Aspartate aminotransferase (AST) in gingival crevicular fluid during experimental periodontitis in beagle dogs, two weeks after ligations. The GCF enzyme levels were 10-100 times higher than in serum. They concluded that the analysis of AST activity in gingival crevicular fluid is an excellent diagnostic indicator of disease activity and treatment efficacy.
Brill & Krasse (1996)[5] conducted a study on GCF in which they introduced filter paper into gingival sulci of dogs that had been previously injected with fluorscein dye intramuscularly. Within 3 minutes, the fluorescent material was recovered on the paper strips. They further conducted studies in humans and proclaimed the crevicular fluid to be a transudate.
Giuuseppe et al (2003)[6] conducted a controlled, short term, longitudinal study to assess the AST activity in GCF during application of continuous orthodontic forces. Distalising force was exerted on one maxillary molar, while the contra lateral & antagonist molars were taken as controls. GCF samples collected from all 3 teeth were analyzed for levels of AST for 4 weeks. They found that AST levels in GCF were significantly elevated in the test tooth after orthodontic forces were exerted on it. This study demonstrated a low increase in GCF AST in teeth with orthodontic appliance, probably due to gingival inflammation produced by plaque-retentive appliance.Different stresses increased the enzyme levels on sites experiencing controlled occlusal trauma (orthodontic forces).Also, more increase was seen on the compression sites than tension ones on the tested teeth.
Perinetti etal (2004)[7] examined colonization of Actinobacillus actinomycetemcomitans, ALP & AST activities in GCF to assess these parameters as biomarkers of tissue responses to tooth movement in humans. The subgingival plaque and GCF around the experimental teeth was harvested from mesial & distal sites immediately before appliance activation and on day 28. Their results suggested that A. actinomycetemcomitans subgingival colonization, ALP and AST activities in GCF reflect the tissue responses that occur in the periodontium during orthodontic treatment.
Aims & Objectives
1. Quantitative estimation and comparison of the Aspartate aminotransferase activity in the gingival crevicular fluid before and during application of orthodontic forces.
2. Investigation of the relationship between wearing of fixed orthodontic appliances and enzymatic changes in the crevicular fluid.
3. Investigation of the relationship between the enzymatic changes in the GCF at the tension and compression surfaces of the tooth undergoing orthodontic movement.
4. Understanding the pattern of variation of enzyme levels during the early period of tooth movement.
Materials & Method
The study was conducted in the Deptt. of Orthodontics & Dentofacial Orthopaedics, Dr Harvansh Singh Judge Institute of Dental Sciences, Panjab University, Chandigarh. A total of 7 female patients requiring orthodontic treatment with first premolar extractions were included in the study. The patients were in good general and periodontal health with all permanent teeth present. The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in 2000.
Serum AST values were obtained for these patients to rule out any systemic disorder which may raise AST values in the GCF.Treatment plan for these patients consisted of fixed mechanotherapy using Pre-adjusted Edgewise appliance (Roth prescription, .022'' x .028'' slot) with extractions of all first premolars.The extractions were done early to allow the enhanced enzyme activity to subside by the time canine retraction was initiated.The first permanent molars were banded and stainless steel brackets were bonded on the central incisors to the second premolars in both upper and lower arches.
After adequate leveling & alignment, the maxillary canines were retracted on 0.018" x 0.025" stainless steel wire using nickel titanium closed coil spring which delivered a constant force of 100 gm. Canine retraction was initiated on randomly selected right maxillary canine (test tooth) while no force was applied on to the left maxillary canine (control tooth.
To ensure optimal plaque control, 15 ml of 0.2% Chlorhexidine gluconate mouthwash was given to each patient, to be used twice daily throughout the study period.Full mouth Plaque Index and Bleeding Index were carried out on the 1st & 28th day of canine retraction to confirm the optimum gingival health throughout the study period.
The GCF was collected using 1μl volumetric micropipettes from mesial & distal gingival margins of maxillary right canine (Test tooth) (Figure 1 and 2) & left canine (Control tooth) at the following intervals-
- before placement of appliance
- at the initiation of canine retraction
- 1st, 7th, 14th, and 28th day after force application
1μl of GCF was made 100 μl with Sorensen's medium containing 0.05% bovine serum albumin in phosphate buffered saline. Samples were centrifuged at 2000 rpm at 4ºC in a refrigerated microcentrifuge for 1 min to remove the bacterial and cellular debris. (Figure 3) The enzyme activity was analyzed using the commercially available quantitative estimation kit (DiaSys, Germany) and UV spectrophotometer (Shimadzu Corp, Japan). (Figure 4)
 | Figure 1: GCF Collection from Mesial Surface of Test Tooth
 |
 | Figure 2: GCF Collection from Distal Surface of Test Tooth
|
 | Figure 3:Refrigerated Microcentrifuge(Sigma Corp, Germany)
|
 | Figure 4: UV Spectrophotometer (Shimadzu Corp, Japan)
|
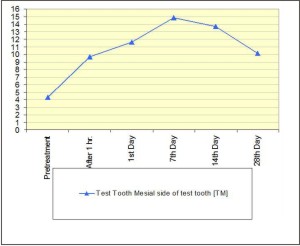 | Figure 5: Mesial side of test tooth (TM)
|
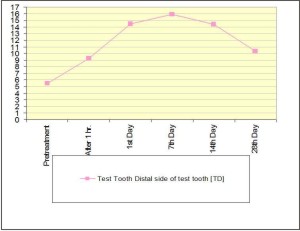 | Figure 6: Distal side of test tooth (TD)
|
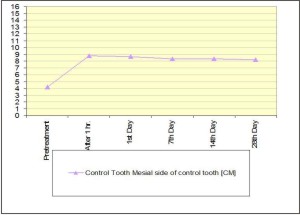 | Figure 7: Mesial side of control tooth (CM)
|
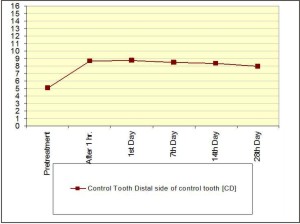 | Figure 8: Distal side of control tooth (CD)
|
 | Figure 9: Comparison Between Mesial and Distal sides of test and control teeth
|
 | Figure 10: Comparison of TM with CM
|
 | Figure 11: Comparison of TD with CD
|
 | Figure 12: Comparison of TM with TD
|
The estimation kit consisted of 2 reagents : Reagent 1 - L-Aspartate +2-Oxoglutarate and Reagent 2 - Oxaloacetate + NADH
Principle of Reaction
L-Aspartate + 2-Oxoglutarate => oxaloacetate + L-glutamate
Aspartate Aminotransferase
Oxaloacetate+NADH => D- malate + NAD + + H +
Malate Dehydrogenase
The GCF AST activity was determined at a constant temperature of 30°C. The diluted sample was mixed with 1000 μl of reagent 1 and incubated for 5 minutes. After this, 250 μl of reagent 2 was added, the absorbance read after 1 minute and subsequently 1,2 and 3 minutes after the 1st reading.
The absorbance was read against air using a quartz cuvette with a path length of 1 cm in the spectrophotometer at a wavelength of 340 nm. The change in absorbance was monitored as the NADH was consumed and ΔA/min was calculated. Absorbance results were converted into enzyme activity by multiplying with the factor specified by the manufacturer at 30 °C (ΔA/min x1513) and expressed as Total AST activity (U/L).
Statistical Analysis
SPSS (Statistical Package for Social Sciences) Program (SSPS Inc, Chicago, USA) was used to perform the statistical analysis. Descriptive statistics such as Mean and Standard deviation were used. For comparisons among and within the groups - Paired t-test, unpaired t-test and ANOVA were used in the study.Plaque Index (PI) and Gingival Index (GI) scores for individual patients were obtained at different time intervals:Before treatment, 1st day of canine retraction (day 0) and 28th day of canine retraction.
Mean and Standard deviation values were calculated for the PI and GI scores.(Table 1)
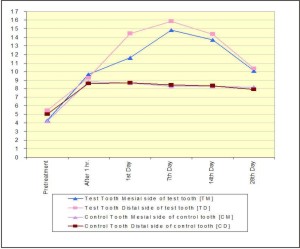
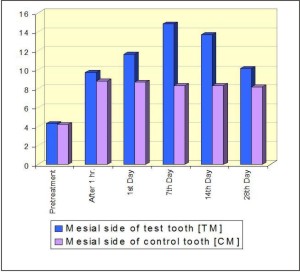
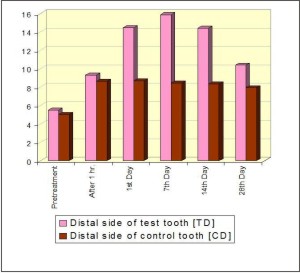
ANOVA test was used to compare the mean values at different time intervals for PI and GI. Paired T-test was used to test the significance of means on day 0 and day 28 for both PI and GI individually. AST activity was assessed for each subject at four sites: test mesial (TM), test distal (TD), control mesial (CM) and control distal (CD) at different time intervals.(Table 2,3,4,5 ; Figure 5,6,7,8,9) Each site was considered as an individual group for statistical comparison.
Comparison among and within the groups was done using Paired and Unpaired t-test.For all the statistical tests that were used to test the significance of difference of means, a 'p' value of less than 0.05 was used for rejection of null hypothesis.(Table 6,7,8,9; Figure 10,11,12,13)
Results
The test teeth underwent a mean distal movement of 1.6 ± 0.4 mm. No significant dental displacement was seen in the control teeth. The serum AST values, taken on day 0 and day 28 showed no statistically significant difference. This indicated that the patients were not suffering from any systemic disorder, which would affect the enzyme values.
Discussion
Our controlled short-term longitudinal study evaluated the GCF AST activity occurring during orthodontic tooth movement, with the aim of evaluating the response of periodontal tissues to orthodontic forces.The change in gingival health due to the introduction of plaque retentive devices (orthodontic appliance) was studied. The GCF AST values after placement of appliance showed a statistically significant change when compared to the values obtained before the treatment was initiated. Therefore, all necessary precautions were taken to maintain the gingival condition throughout the study period.
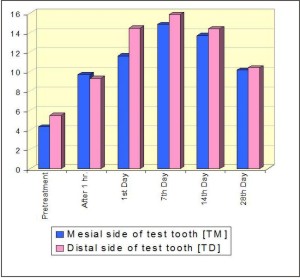
The GCF AST activity values were found to be higher on the mesial and distal surfaces of the test tooth (TM and TD) (Table 8 ; Figure 12) as compared to the mesial and distal surfaces of the control tooth (CM and CD) (Table 9 ; Figure 13) on day 0.This was due to the early inflammatory response due to the controlled occlusal trauma exerted on the test tooth by orthodontic forces. AST activity peaks were seen in the TM and TD group on 7th day. This AST activity elevation could be a consequence of tissue remodeling due to the orthodontic forces. Reitan et al[2] had shown that cell necrosis was seen as a result of mechanical stress on periodontal ligament and alveolar bone.The GCF AST activity increased on both the tension (TM) and compression (TD) sites on the 1st day after initiation of canine retraction. This coincides with the initial phase of tooth movement, where there is tissue destruction all around the tooth being moved.In contrast, the enzyme values on the control tooth did not show a significant increase on the 1st day, due to absence of significant occlusal trauma.
The enzyme activity increased significantly on both mesial and distal surfaces by the 7th day, suggesting presence of cell destruction during active tooth movement on both the tension and compression sites. Again no significant change was observed on the control tooth. These results are in agreement with the study by Giuuseppe et al[6]. By the 14th day, the enzyme values reduced on both the tension side (TM) and the compression side (TD), but were higher on the compression side. This implies that more periodontal tissue destruction was occurring on the compression side.The enzyme values did not show any such change on the control tooth.
In the study conducted by Perinetti et al [7], the enzyme levels were at peak on both mesial & distal sides of test tooth on the 14th day. This indicates maximum cellular response on both sides on the 14th day.Therefore, further investigation needs to be conducted to periodically examine the enzyme levels on pressure and tension sites.
On the 28th day, the values significantly decreased on both the TM and TD sites, suggesting a reduction in cell destruction. This period coincides with the post-lag phase of tooth movement. Whereas, the enzyme activity at the control sites was still comparable to those at the time of initiation of canine retraction. These values indicate that the cellular activity may be less destructive in nature after 28 days while continuous forces are maintained, leading to reduction in the enzyme values. Nevertheless, these values still remained above baseline values.
Conclusion
1. Aspartate aminotransferase can be successfully estimated in the gingival crevicular fluid during orthodontic tooth movement.
2. An increase in the GCF AST values collected from all the surfaces was observed after placement of orthodontic appliance. This confirmed that the presence of fixed orthodontic appliance lead to deterioration of the gingival condition.
3. Orthodontic forces were responsible for increased tissue destruction in the periodontal tissues. This is shown by the significant rise in the level of AST enzyme activity in the GCF on test teeth as compared to the control teeth.
4. The enzyme activity was more at the compression surface than at the tension surface on the 1st, 7th & 14th days. Thus, there was increased destruction of the periodontal tissues on the compression surface.
5. There was a definite pattern of enzyme activity during orthodontic tooth movement with the peak of enzyme activity occurring on the 7th day at the tension and compression surfaces of the test tooth.
6. AST activity shows little inter-patient variability in terms of rise and falls of level of the enzyme.
Thus, within the limitations of the present study, GCF AST activity can be proposed as a sensitive biomarker of the periodontal metabolic changes during orthodontic tooth movement.
References
1. Karmen A . A note on the spectrometri assay of glutamic-oxalacetic transaminase in human blood serum. J Clin Invest. 1955 Jan;34(1):131-3.
2. Reitan K .The initial tissue reaction incident to orthodontic tooth movement as related to the influence of function; an experimental histologic study on animal and human material. Acta Odontol Scand Suppl. 1951;6:1-240
3. Lilja E S. Lindskog L. Histochemistry of enzymes associated with tissue degradation incident to orthodontic tooth movement American Journal of Orthodontics Volume 83, Issue 1 , Pages 62-75, January 1983
4. Cohen R L, Crawford M E , McSwiggin T , Chambers D A. Association of gingival crevicular fluid aspartate aminotransferase levels with histopathology during ligature-induced periodontitis in the beagle dog. J Dent Res. 1991 Jun;70(6):984-7.
5. Krasse B. Serendipity or luck: stumbling on gingival crevicular fluid. J Dent Res. 1996 Sep;75(9):1627-30
6. Giuuseppe P, Miichele P, Miichele D et al. Aspartate Aminotransferase Activity in Gingival Crevicular Fluid during Orthodontic Treatment: A Controlled Short-TermLongitudinal Study. J Periodontol 2003; 74: 145-152.
7. Perinetti et al . Longitudinal monitoring of subgingival colonization by Actinobacillus actinomycetemcomitans, and crevicular alkaline phosphatase and aspartate aminotransferase activities around orthodontically treated teeth. Journal of Clinical Periodontology 2004;31:60-67. |