Introduction
The production of local anesthesia in the mandibular branches of trigeminal nerve is essential for many dental procedures. The most widely used technique for achieving mandibular nerve anesthesia through the world is direct conventional inferior alveolar nerve block technique along with lingual and long buccal nerve block technique. This is an open mouth intraoral approach allowing easy and accurate insertion of needle. However, this technique has its own drawbacks like anatomical variation of mandibular foramen which may make accurate localization of mandibular foramen difficult. Also requires a separate injection technique for long buccal nerve.[1] The Gow-Gates and Akinosi techniques are both 'high' methods of blocking the inferior alveolar nerve, both anesthetize the lingual nerve also. The Gow-Gates and Akinosi methods are best reserved for those cases where the conventional methods fail.[2]
Akinosi introduced the technique for mandibular anesthesia in 1977. However Vazirani also described similar technique in 1960; hence the name was changed to Vazirani Akinosi technique. The injection is a closed mouth technique, with the landmarks for needle insertion being the mucogingival junction of the maxillary second molar.[3] The aim of the study is to evaluate the anesthesia of long buccal nerve in the Akinosi mandibular closed mouth technique.
Materials And Methods
The study group consisted of 100 patients who reported to the Department of Oral and Maxillofacial Surgery in D.J. College of Dental Sciences and Research programmed for lower molar extractions (55 males and 45 females) and who gave their informed consent to participation. In all cases injections of 1.8 ml of 2% lidocaine with adrenaline 1:2, 00,000 using 26 gauge and 38mm long needle disposable syringe were used. In the event buccal or lingual anesthetic reinforcement proved necessary, 1ml of anesthetic solution was instilled at each reinforcement point. In cases where Akinosi closed mouth nerve block was not working, standard inferior alveolar nerve block was given and these cases were regarded as failures. All procedures were carried out by same professionals. [4]
Inclusion And Exclusion Criteria For Study
Inclusion Criteria
Between the ages of 15 and 72 years
Possess mandibular molars
Informed written consent given before participation
Exclusion Criteria
Allergies to local anesthetics or sulfites
Pregnancy
Inability to breathe through nose
History of significant medical conditions
Taking any medications that might affect anesthetic assessment and pain perception (non steroidal anti- inflammatory drugs, opoids, antidepressants, alcohol)
Active site of pathosis in area of injection
Inability to give informed consent[5]
Hundred patients received the Vazirani -Akinosi nerve block described by Akinosi and Vazirani. The patients were in supine position and asked to bring teeth in occlusion, with the muscles of mastication relaxed. The cheek was retracted laterally. The injection site was the soft tissue overlying the medial surface of ramus, adjacent to maxillary tuberosity, at height established by the mucogingival junction in the area of the maxillary second molar. The syringe was held parallel to maxillary occlusion plane and directed posteriorly. The needle penetrated the mucosa and then was advanced slowly to a depth of approximately 30mm in the pterygomandibular space. Aspiration was performed, and 1.8ml of anesthetic solution was deposited during the period of two minutes.[3] After 5-7min of the injection, the anesthesia of the tissue innervated by the sensory oral branches of the mandibular nerve was tested using a pinprick on the following area as of the corresponding side: buccal mucosa adjacent to the mandibular molar, buccal mucosa adjacent to the canine and dorsal side of tongue. Presence of pain sensation was assigned as 1 and absence of pain sensation was assigned as 0. Aspiration was rated as 0=negative; 1=positive (blood aspiration)
Patients who did not experience numb lip and tingling sensation of tongue on the corresponding side and experience severe pain at the commencement of tooth extraction were counted as failures.[6]
Results
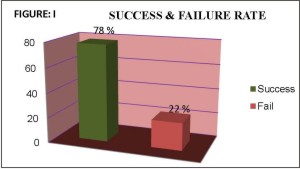
Subjective symptoms were evaluated 5-7min after Akinosi closed mouth nerve block. The initial manifestation of anesthesia consisted of tingling and numbness of lower lip and tongue. A total of 22 patients out of 100, did not have profound lip numbness and tingling of tongue .In 78 patients pain prick sensation was not present on examining the buccal aspect of canine and on the lingual aspect. The failure rate evaluated was 22 % (Figure: 1).
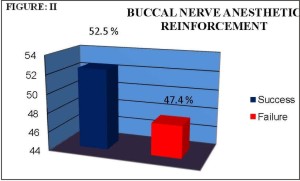
In 41 patients, no pain prick sensation was present on the buccal aspect of the molar(52.4%) while in 37 patients pain was present on the buccal aspect of the molar (47.4%) so a separate buccal nerve reinforcement was required (Figure: 2).
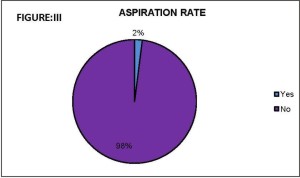
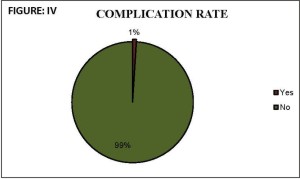
Positive blood aspiration was noted in 2 out of the 100 infiltrations (2%) (Figure: 3). One out of 100 patients anesthetized with the Akinosi closed mouth technique claim to be unable to close an eye, though this problem rapidly subsided(transient facial nerve paralysis) (Figure: 4).
 |
 |
 |
|
 |
|
 |
|
Discussion
Local anesthesia is essential for pain free dentistry, yet intra-oral injections often are considered painful and a source of anxiety for many patients. Anesthesia for mandibular procedures may be achieved by using standard inferior alveolar block, the Gow-Gates or Vazirani-Akinosi techniques. The latter two techniques, which have unique insertion points and paths, are being used increasingly, as they have specific advantages over traditional standard block.[5]
The indications of Akinosi technique are, limited mandibular opening, multiple procedures on mandibular teeth, inability to visualize landmarks for inferior alveolar nerve block, because of large tongue.
It is thought that this technique may be less threatening to patients because the patient does not have to open their mouth. It is relatively atraumatic and has fewer postoperative complications like trismus. It provides successful anesthesia where bifid canals are present. It has faster rate of onset, decreased psychological stress for anxious patients and ease of administration. It can be used for patients with a strong gag reflex and in patients with macroglosia. There is decrease pain on injection, because tissues are relaxed . However there are some disadvantages of this technique such as difficulty to visualize the path of the needle and depth of injection.It is difficult in patients with widely flaring ramus, pronounced zygomatic ridge or internal oblique ridge. It has no bony contact, depth of penetration somewhat arbitrary and potentially traumatic if needle is too close to periosteum.[7]
An anesthetic effect was achieved in all of the patients subjected to the Akinosi technique if the proper technique was used.[4] In our study, twenty two of these patients, no effect was achieved after waiting for 10 minutes following infiltration of the anesthetic solution using Akinosi technique. These cases were counted as failures. In these cases a separate classical inferior alveolar nerve block was given. Hence incidence of inferior alveolar nerve block and lingual nerve anesthesia with single needle puncture was found to be 78% in our study.
Sisk reported a faster onset of anesthesia with Akinosi technique (in 90% of cases) compared with the conventional technique (85%). As onset of anesthesia depends on the closeness of approximation of the nerve blocking drug to the related nerve trunk, it is possible that the failure of anesthesia may be due to not depositing anesthetic solution in the near proximity of the oral sensory branch of the mandibular nerve in the pterygomandibular space.[7]
Negative aspiration in the Akinosi technique suggest a lack of sizeable blood vessels in the mid portion of the pterygomandibular space.[6] According to Martinez-Gonzalez needle aspiration proved positive in 4% of the patients anesthetized with the Akinosi technique.[19] In our study 2% positive aspiration was noted.
Akinosi and Gustainis and Peterson indicated that the Akinosi technique only requires one injection to achieve anesthesia of the mandibular nerve; in our series, however, 47.4% patients required two injections to achieve complete anesthesia and in 52.4% patients only one injection was required. Thomas A. Johnson reported that the Akinosi technique like the Gow-Gates block the long buccal obviating the need for a separate injection. Refua reported that long buccal nerve anesthesia is higher in Akinosi technique. Similar results was given by Gautam A. Madan that this technique block the long buccal nerve in some cases so a separate nerve block is required to achieve anesthesia. Although Vazirani-Akinosi technique may sometime require additional injection to buccal nerve but where it is not required, extra dose of local anesthetic required is reduced.[1]
Gautam A Madan, J.G Meechan reported that no bony landmark is available in this technique. Hence, a small chance exists of over inserting the needle and injuring the vessels in the pterygoid plexus. Hence, closed mouth block is reasonably safe technique to achieve mandibular anesthesia[1]. In our study one out of 100 patients anesthetized with the Akinosi closed mouth technique claim to be unable to close an eye (transient facial nerve paralysis), though this problem rapidly subsided.. In our study, possibly 7th nerve palsy occurred due to over insertion of needle and deposition of anesthetic solution deep in to the parotid gland.
Conclusion
Our experience suggests that Vazirani-Akinosi technique permits an effective anesthesia of inferior alveolar, lingual and buccal nerve to be obtained in single injection in statistically significant number of cases. Supplemental buccal nerve block may be necessary in some cases.
References
1. Verma Nitin, Lata Jeevan "Comparison and Clinical Efficacy of Mandibular Nerve Anesthesia by Direct Conventional Technique with Vazirani-Akinosi Mandibular Nerve Block Technique." J Anaesth Clin Pharmacol 2010; 26(1): 79-82.
2. J.G.Meechan. "Anesthesia: how to overcome failed local anesthesia." British Dental Journal 1999; 186:15-20.
3. Steven Goldberg, Melissa Drum, John Nusstein, Mike Beck. "Comparison of the anesthetic efficacy of the Conventional inferior, Gow-Gates, and Vazirani-Akinosi Techniques." Journal Of Endodontics 2008;34(11):1306-1311.
4. Martínez-gonzalez jm, benito-pena b, fernandez-ca-liz f, san hipolito-marín l, penarrocha-diago m. "A comparative study of direct mandibular nerve block and the Akinosi technique." MED ORAL 2003; 8:143-9.
5. Shawn jacobs. "Injection pain: comparison of three mandibular block techniques and modulation by nitrous oxide and oxygen." JADA 2003; 134: 869-876.
6. Todorovic l., stajcic z. And petrovic. "Mandibular versus inferior dental anesthesia: clinical assessment of #different techniques." IJOMS 1986; 15:733-738.
7. Sisk Al. "Evaluation of the Akinosi mandibular block technique in oral surgery." Jr. Oral and Maxillofacial Surgery". 1986; Feb 44(2): 113-5.
8. Akinosi J.O "A new approach to the mandibular nerve block." Br. J. Oral Surgery, 1977;15(1):83-87.
9. Alantars.A, Lefevre B, Misipo E "The Akinosi dental anesthesia technique: apropos of 10 clinical cases." Actualités odonto-stomatologiques 1991; 45(173):121-130.
10. Cruz ev, quengua jb, guitierrez il, abreau ma, uy hg. "A Comparative study: classical, Akinosi, and Gow- Gates technique of mandibular nerve block." J Phiillipp Dent Assoc. 1994 ; 46(1):13-19.
11. Aggrawal vivek, Singla M, Kabi D. " Comparative evaluation of anesthetic efficacy of Gow Gates mandibular conduction anesthesia, Vazirani - Akinosi technique, buccal- plus- lingual infiltrations, and conventional inferior alveolar nerve anesthesia in patients with irreversible pulpitis." Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Feb; 109(2): 303-8.
12. Malamed stanley f. "Handbook of Local Anesthesia", Fifth edition 2007. |