Introduction
Over the past few decades a considerable reduction in caries experience has occurred in the pediatric and adolescent population in the developed countries. Smooth surfaces, especially inter proximal surfaces, have benefitted to a great extent from the caries preventive effects of various fluoride agents but caries in pits and fissures have received minimal advantage from them. The extreme vulnerability to decay of occlusal surfaces has prompted dental scientists to seek methods of caries prevention especially for pits and fissures. The culmination of these efforts has resulted in the current technique of occlusal sealing.
The long-term efficacy of sealants is well documented in numerous research work done over the years.[1] In spite of convincing evidence of the ability of fissure sealants as a preventive and cost effective method of caries prevention, the dental community still eyes it with reservation.[2]
Various techniques which may augment the sealant retention have been proposed. Among them prophylaxis, air polishing, air abrasion and opening the fissure with the bur have been attempted. In addition use of an intermediate bonding layer before placement of sealants has been advocated in recent studies.[3] No studies till date is conclusive regarding the appropriate technique of tooth preparation and use of bonding agent in reducing the microleakage and improving the long term clinical retention of fissure sealants.[4][5] Contradictory results of the previous studies kindled us to conduct the present investigation to compare the effectiveness of different methods of cleaning and preparing occlusal fissures with/without bonding agent prior to pit and fissure sealant placement so as to improve the long term clinical efficacy.
Material and Methods
The present study was designed to compare and evaluate microleakage in commonly used pit and fissure sealant using different methods of cleaning and preparing enamel surfaces. The effect of application of the bonding agent was also evaluated.
Forty caries free human permanent first maxillary premolars freshly extracted for orthodontic purposes were selected for the study.
The specimens were cleaned and debrided under tap water and any periodontal tissues attached to the roots of the teeth were removed with a periodontal scaler. After cleaning the specimens were stored in 0. 1% thymol solution until further use.
The specimens were randomly divided into 4 groups of 10 teeth each.
Prophylaxis Group (Py) - Teeth were cleaned with pointed bristle brush for 10 seconds using a slow speed hand piece.
Air polishing Group (Ap)-Air polishing unit (EMS AirFlow Handy Nyon, Switzerland) was used to prepare fissures by delivering air powered slurry of warmed water and sodium bicarbonate with the nozzle at 90 degree, pressure of 3.5-4.5 bars and at the rate of 18-80 ml /min as per manufacturer's instruction.
Air Abrasion Group (Ab)-Air abrasion was used to prepare fissures. Air sonic mini airblaster (Bio-art, Sao Carlos Brazil) with 50µm alumina particle size and 80psi pressure was kept at a distance of about 5cms from the tooth surface with the nozzle at 120 degree to the tooth surface using irregular movements and rapid trajectories as per manufacturer's instruction.
Invasive Group (Iv)- The teeth were prepared using ¼ round carbide bur (.005) (SS White) in a high speed handpiece so as to open the fissures to the depth and width of the bur head.
The teeth were acid etched using 35% phosphoric acid (Denfill, Verrcom Dental Materials, Korea) for 15 seconds[6] and rinsed for 10 seconds using water spray of three way syringe. They were blot dried for sixty seconds and further divided into 2 subgroups comprising of bonded and nonbonded subgroups of five teeth each. In bonded subgroups (Py1, Ap1, Ab1, Iv1) two layers of bonding agent (Adper TM Single Bond 2 Adhesive,3M ESPE St Paul, MN, USA) was applied. Excess bond was air dried gently for 5 seconds and light cured for 10 seconds. In all 8 subgroups (Py1, Py2, Ap1,Ap2, Ab1,Ab2,Iv1and Iv2) pit and fissure sealant (ClinproTMsealant,3M ESPE St Paul, MN, USA) was applied as per manufacturer's instructions. Any obvious voids were removed with a 0.5mm tip diameter periodontal probe. Polymerization was done using visible light cure (Hilux LED Max4) for 20 seconds, with the tip of the curing light held vertical to the resin surface and about 1mm away. The margins of the sealant were checked for proper intactness and retention with an explorer
The specimens were incubated in distilled water at room temperature for 24 hours. Thermocycling was performed at 5º, 37ºand 55º for 500 cycles with a dwell time of 30 seconds in each bath to simulate the oral environment.
Microleakage Detection
Two coats of acid resistant varnish were applied to all tooth surfaces exposing 1mm enamel around periphery of sealant. The apices of the roots were sealed with sticky wax.
The samples were then immersed in 1% aqueous solution of fluorescent acridine orange dye (Otto Kemi, Mumbai, India) for twenty four hours, following which the samples were washed to remove excess dye. The specimens were embedded in acrylic blocks up to cementoenamel junction and longitudinal sections in buccolingual directions of 1mm were made with water cooled diamond disc. The sections were kept dry and were examined under fluorescent microscope (Lawrence and Mayo) to study microleakage with magnification at 10 X. The degree of microleakage was scored by a single observer according to the scoring criteria by Cooley RL, et al., [7] [Table1]
The sections were photographed to show microleakage with score of '0', '1', '2' and data was statistically analyzed.
Statistical Analysis
Data was presented as scores corresponding to the microleakage. SPSS software (Version 9.0) was used for the statistical analysis. Difference between the groups was assessed by using chi-square test.
Results
Intercomparison between the bonded and the nonbonded similar sub-groups reveal no significant difference except between Py1 and Py2 subgroups (p<0.005) (Graph 1). Intra comparison between the bonded subgroups revealed no significant difference between them (Table 2). While, intracomparison between the nonbonded subgroups showed significant difference between the prophylactic (Py2) and invasive (Iv2) subgroup (p<0.005) (Table 2).
Multiple statistical intercomparisons between the subgroups revealed no significant difference between the bonded prophylactic subgroups (Py1) and other nonbonded subgroups (Table 2). Comparison of airpolishing (Ap1) bonded subgroups with other nonbonded subgroups revealed significant difference with Py2 and Ab2 except Iv2. Comparison of Ab1 with other nonbonded subgroups revealed significant difference with Py2 and Ap2 except Iv2. However on the contrary , the bonded invasive subgroup(Iv1) showed a significant difference with all the nonbonded subgroups(Py2,Ab2,Ap2) .Highly significant difference was observed between invasive with
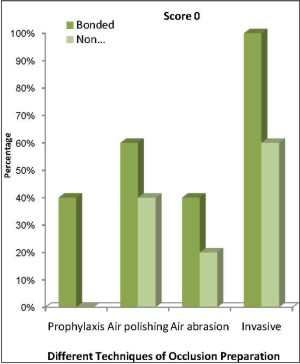 | Graph 1- Comparison Of Microleakage For Score 0 (no microleakage) Between Bonded And Nonbonded Groups.
 |
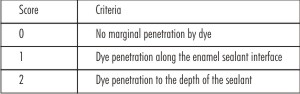 | Table 1-Cooley’s scoring criteria for microleakage
|
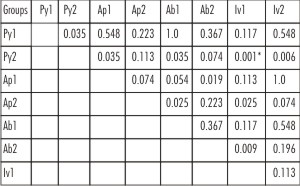 | Table 2-Multiple Statistical Comparisons Of Microleakage Score Among Subgroups
|
bond(Iv1) and prophylactic without bond subgroup(Py2) (Table-2)
Chi square test where p≤0.05 Significant, p ≤ 0.001 Highly Significant, p>0.05 Non significant
Represents statistically significant difference between compared subgroups.
Represents highly significant difference between compared subgroups
Discussion
Since the advent of the 21st century, dentistry is moving towards an era of preventive and minimally invasive dentistry. This can be attributed to availability of newer restorative materials with better adhesive properties. It is now quite evident that sealants are one of the best methods to prevent dental
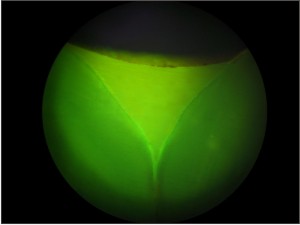 | Figure 1- Section showing no microleakage-score 0
|
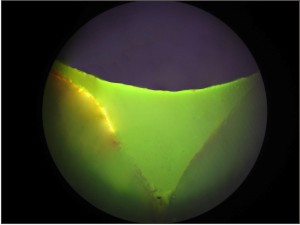 | Figure 2-Section showing microleakage with dye penetration along the enamel sealant interface -score 1
|
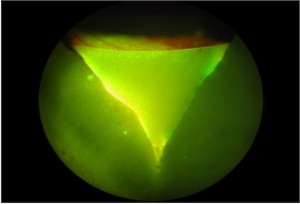 | Figure 3-Section showing microleakage with dye penetration to the depth of the sealant -score 2
|
caries and to arrest the further growth of incipient caries.[8] However long term clinical success of sealants is related to their proper handling.[9] The clinician has a choice of using different methods of enamel preparation which can improve the retention and adaptation of the sealant and in consequence improve its longevity. Previous studies have indicated that application of bonding agent enhances the marginal adaptation of sealants and can be used as a golden standard.[10] However none of them have clearly specified the most optimal method of enamel preparation before application of the bonding agent. Microleakage is one of the parameters which help in assessing the marginal adaptation and can aid in arriving at the most effective method of occlusal preparation.
Despite the fact that a self etch bonding requires less time, in the present study, separate etch and bonding system was preferred since acid etching followed by rinsing removes the prismless layer and causes sufficient microretentive bonding of the sealant.[11] Self etching increases microleakage, lowers bond strength and creates etching pattern not deep enough for bonding of the resin.[12]
In the present study it was observed that the prophylaxis group showed highest microleakage with maximum sections of dye penetration to the depth of fissure. The possible cause could be that a rotating bristle brush is unlikely to clean the acquired pellicle from fissure embrasures as the bristles sweep across the inaccessible regions and polish the more exposed superficial regions. [13]
Both air abrasion and air polishing are minimally invasive procedures causing little change in the microscopic surface structure. The present study showed better marginal integrity with air abrasion and air polishing method .The present findings were concurrent to a similar studies by Garcia Goday et al., [14] Chan et al[15], Knobloch La et al[16].These procedures create a roughened surface, increasing the surface area for sealant. Both the methods yielded similar results which could be attributed to similarity between the two techniques.
The invasive group in the present study showed best marginal integrity. These results were in agreement with previous studies.[14],[17],[18] The probable reason could be that widening and deepening of the fissure eliminates organic material and plaque, increases surface area and removes superficial layer of aprismatic enamel present at the base of the fissure. These results were contrary to studies conducted by Blackwood JA et al.,[19] and Srinivasan Vet al.,[20] who reported that marginal seal was unaffected by different methods of enamel preparation. Possible cause could be the difference in the method of evaluation of microleakage. In the present study fluorescent dye penetration method that has been tried, is extremely sensitive to ultra violet light ,shines brightly even in areas of low molecular concentration and can easily penetrate microscopic spaces in the cavosurface resin /enamel interface [21]
Application of the bonding agent showed increase in marginal adaptation in all groups. Similar findings were also observed in previous studies where application of bonding agent showed improved microleakage, shear bond strength and better vertical penetration.[22],[23] The benefit of this primer and adhesive layer under the sealant is based on a combination of moisture-chasing effects of the hydrophilic primers, increased flow imparted by the less viscous primer and adhesive, and increased flexibility of the combined polymerized primer / adhesive / resin complex leading to a better initial bond and a more resilient long-term bond. [24]
However on the contrary no difference in sealant retention with or without bonding agent was reported in studies by Ana Karina Mascarenhas et al., [25] and Pinar A et al., [26] This variation could be attributed to difference in the type & technique of bonding agent applied and the fluorescent dye penetration technique used for evaluation of microleakage.
The effect of bonding agent on the level of microleakage with respect to various enamel preparation groups was variable. Bonding agent demonstrated a marked decrease in microleakage in noninvasive methods like prophylaxis, which showed extensive microleakage before its application, whereas minimally invasive and invasive methods of enamel preparation showed lesser degree of decline in the same suggestive of the fact that minimally invasive and invasive preparations may not routinely necessitate an intermediate layer of bonding.
Conversely, microleakage in invasive subgroup without bond was comparable to minimally invasive subgroup of air abrasion and air polishing with bond .Similarly microleakage in non-invasive prophylaxis with bond was comparable with minimally invasive subgroup of air abrasion and airpolishing without bond. This could be due to additive effect of bonding agent being used.
Within the limitations of the present study, it can be suggested, that a judicious use of various techniques of occlusal preparation can guarantee long term success of sealants. Minimally invasive methods are the best choice for enamel preparation while, the invasive method should be restricted to questionable pit and fissures and should be restored with a preventive resin restoration wherever indicated.
In the event of an uncooperative patient, newly erupted teeth, or unavailability of equipment for minimally invasive treatment/therapy, non invasive method of enamel preparation with a bonding agent could be preferred without compromising the success of the sealant. Though the present investigation evaluated the microleakage between various tooth preparation techniques other factors such as pull-out strength and shear bond strength which determine the longevity of the sealant need to be further instigated. Further long term studies with larger sample size are dictated to evaluate fissure sealant techniques both in the laboratory as well as in clinical trials.
Conclusion
Fissure sealants are likely to play an important role in caries prevention and will augment fluoride and other techniques that are intended to protect caries susceptible surfaces. To improve marginal adaptation of the sealants, minimally invasive methods are the most favoured method of occlusal preparation. Application of a bonding agent in addition to simple procedures like prophylaxis may improve the marginal integrity of a sealant resulting in their long term retention. The above results may be viewed as guidelines which will help dentists to standardize the appropriate sealant placement technique, so as to harness the effectiveness of this restorative procedure within the realm of preventive philosophy.
References
1. Simonsen RJ: Retention and effectiveness of dental sealant after 15 yrs: Amer Dent Assoc,1991: 122 :1: 42-43
2. Robert J. Feigal Sealants and preventive restorations: review of effectiveness and clinical changes for improvement .Pediatr Dent 1998-20 ;2;85-92
3. Borem ML and Fiegel RJ. Reducing microleakage of sealant under salivary contamination. Digital image analysis evaluation. Quintessence Int 1994; 25: 283-289
4. Agrawal A, Shigli A. Comparison of six different methods of cleaning and preparing occlusal fissure surface before placement of pit and fissure sealant: An in vitro study J Indian Soc Pedod Prev Dent 2012 ;30 :1:51-5
5. Nejad SJ, Razavi M, Birang R, Atefat M. In vitro study of microleakage of different techniques of surface preparation used in pits and fissures. Indian J Dent Res 2012;23: 24:7-50.
6. Nordenvall KJ, Brannstrom M, Malmagen O. Etching of deciduous teeth and young and old permanent teeth. A comparison between 15 and 60 seconds of etching. Am J Orthod ;1980 :78: 99-108
7. Cooley RL, McCourt JW, Huddleston AM, Casmedes HP. Evaluation of fluoride containing sealant by SEM, microleakage and fluoride release. Pediatr Dent 1990, 12: 38-42.
8. Simonsen RJ, Neal RC.A review of the clinical application and performance of pit and fissure sealants. Aust Dent J. 2011 Jun;56 Suppl 1:45-58
9. BarrossoJM, LessaFC, Palma DibbRG ,torres CP,Pecora J , Borsatto MC. Shear bond strength of pit and fissure sealants to saliva contaminated and non contaminated fissures J Dent Child 2005 ;72:95-9
10. Marie-Eve Asselin, Daniel Fortin,YvesS!tbon, Pierre H. Rompre. Marginal Microleakage of a Sealant Applied to Permanent Enamel: Evaluation of 3 Application Protocols Pediatr Dent 2008 :30 :1;29-33
11. Kanemura N, Sano H, Tagami J. Tensile bond strength to and SEM evaluation of ground and intact enamel surfaces. Journal of Dentistry 1999;27(7):523-30
12. Perry AO, Rueggeberg FA The effect of acid primer or conventional acid etching on microleakage in a photoactivated sealant. Pediatr Dent 2003;25;2:127-31
13. Donnan MF and Ball IA. A double blind clinical trial to determine the importance of pumice prophylaxis on fissure sealant retention. Br Dent J 1988; 165: 283-285.
14. Garcia-Godoy F and Medlock JW. An SEM study of the effects of air polishing on fissure surfaces. Quintessence Int 1988; 19;7: 465-467.
15. Chan DCN, Summit JB, Garcia Goday F, HiltonTJ, ChungKH. Evaluation of different methods of cleaning and preparing occlusal fissure. Oper Dent 1999; 24: 331-336.
16. Knobloch LA, Meyer T, Kerby RE, Johnston W. Microleakage and bond strength of sealant to primary enamel comparing air abrasion and acid etch techniques. Pediatr Dent. 2005 ; 27:6:463-9.
17. Joseph S, Eidelman, Dr. Odont. Six year evaluation of fissure sealants placed after mechanical preparation. A matched pair study. Pediatr Dent 1986; 8: 204-205.
18. In vitro evaluation of microleakage under a glass ionomer surface protector cement after different enamel treatment procedures. Haznedaroglu E, Mentes AR, Tanboga Oral Health Dent Manag. 2012 ;11;1:16-22.
19. Blackwood JA, Dilley DC, Roberts MW, Swift EJ Jr. Evaluation of pumice, fissure enameloplasty and air abrasion on sealant microleakage. Pediatr Dent 2002; May-Jun 24(3): 199-203.
20. Srinivasan V, Deery C, Nugent Z In vitro microleakage of repaired fissure sealant. A randomized, controlled trial. Int J Pediatr Dent 2005; 15 ;1: 51-60.
21. Alpino PHP and Pereira JC. Use of fluorescent compounds in assessing bonded resin based restorations: a literature review. J Dent 2006; 34: 623-634
22. Choi JW, Drummond JL, Dooley R. The efficacy of primer on sealant shear bond strength. Pediatr Dent 1997; 19: 286-288
23. Tulunoglu O, Bodur H, Uctasli M, Alacam A. . The effect of bonding agents on the microleakage and bond strength of sealant in primary teeth. J Oral Rehabil.1999;26:436-441
24. Symons AL, Chu CY, Meyers IA. The effect of fissure morphology and pretreatment of the enamel surface on penetration and adhesion of fissure sealants. J Oral Rehabil. 1996;23:791-798.
25. Ana Karina Mascarenhas, Huda Nazar, Sabiha Al-Mutawaa, Pramod Soparkar, Effectiveness of primer and bond in Sealant Retention and Caries Prevention. Pediatr Dent;30(1)08,25-8
26. Pinar A, Sepet E, Aren G, Bölükba?i N, Ulukapi H, Turan N Clinical performance of sealants with and without bonding agent. Quentessence International 2005;36:355-60 |