Introduction:
Radiography is an important diagnostic aid in medical and dental practice. Radiographic procedures offers obvious advantages in diagnosis of physical abnormalities associated with speech because they allostructures normally hidden from view to be visualized. One can make a complete palato-pharyngeal analysis on the basis of a simple lateral radiograph[4] or obtain even more accurate information from a cephalometric tracing. The various characteristics that can be adequately analyzed are
i) Soft palate length, thickness, size of levetor eminence and position of rest.
ii) Hard palate length and relation to arch of atlas.
iii) Nasopharyngeal antero-posterior dimension and lateral dimension.
The first use of X-ray technique in speech research was by investigators whose primary interest was in phonetic definition. The early work of such researchers as Russel[5],[6] in 1928 and Trevine[7] in 1932 was reviewed by McMilan and Kelemen[8] in 1952 and Subteley[9] in 1957. On the basis of these investigations, it was established that certain consistent interrelationships exist among the articulation and sounds in speech production. In 1931, Broadbent[10] presented a technique that standardized roentgenigrams of the head and signaled the beginning of cephalometricroento genelogy, and in 1955 Suntelny[11] confirmed the width of the nasopharynx was significantly greater than normal in patients with cleft palate.
The information obtained from the single exposure process is invaluable to the current understanding of velopharyngeal closure. There are certain advantages
This method is economical.
The patient is not required after the radiograph is taken for the analysis.
According to S.A Jakhi and F.R Karjodhar[12] there is increase in the width and depth of nasopharynx, with a consequential increase in pharyngeal cavity volume in patients with cleft palate speech when compared with normal speech and with nasality.
Other important techniques employed in speech research are laminography[13], cineradiography[14], videonasophary ngoscopic[15] and high speed motion picture techniques. Recently a computer controlled radiographic technique called the X-rays microbeam system has been developed[16], [17]. Although this technique holds much more promise and it is extremely expensive.
Change in levatorvelipalatini muscle activity for patients with cleft palate in association with placement of speech-aid prosthesis[18], [19]. In this year Ueda N et al[20] created a new Palatal Lift Prosthesis was also found to be effective in patients with cleft palate with a short clinical crown.
The planning of the surgical procedure, in order to match the postoperative structure to the preoperative velopharyngeal dimensions and movements visualized through Videonasopharyngoscopy and videofluoroscopy, seems to be the most important aspect of the surgery for correcting residual velopharyngeal dysfunction[21].
For the purpose of the study is to find a simpler technique in diagnosis of speech disorders. So we were used lateral cephalogram as a diagnostic method for speech disorder in cleft palate patients.
Materials And Method:
A study focused on a sample of 60 patients consisting of group A, 20 patients with unrepaired cleft palate speech; group B, 20 patients with repaired cleft palate speech; and group C, 20 patients with normal speech. The patients were selected in consultation with a speech pathologist in ALL INDIA INSTITUTE FOR SPEECH AND HEARING, MYSORE and the sample of speech was analyzed on a speech spectrograph using PRAAT SOFTWARE.
The age of the patients in each group ranged from 5years to 25years (27 males and 33 females). All the patients were of average socioeconomic status and Indian origin. According to basic criteria of selection, none of the subjects had received orthodontic treatment, the adult had all teeth up to the second permanent molar, and the children had all the teeth up to the second deciduous molar. Subject who had undergone adenoidectomy were not included in the study. The specific criteria for selection of subjects in each group were as follows:
GROUP A-(8 males and 12 females)
1. All patients had unrepaired incomplete cleft palate speech.
GROUP B-(9males and 11 females)
1. All the patients had repaired unilateral incomplete cleft palate speech.
GROUP C-(10 males and 10 females)
1. All the patients had angle Class I occlusion.
2. Slight crowding among lower anterior teeth was considered within normal.
3. Palate was normal.
4. Speech was normal.
Standard lateral head roentgenograms were taken from the cephalostat in accordance with the standard cephalometric procedures. Data on the oral and pharyngeal cavities were recorded with respect to landmarks presented by Proffit and Mcglove[1], Proffitet al[2], and Ricketts.[3] Upper impressions were taken and casts were prepared and first and second molar widths were measured with Vernier caliper.
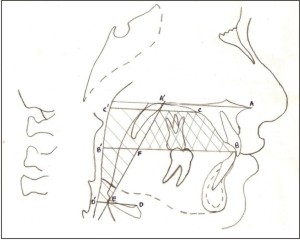 | Fig.1. Cephalometric Landmarks, Planes Used In Study Of Oral Cavity Area And Pharyngeal Cavity Area.
 |
Oral and pharyngeal cavities (Fig. 1)
Fig. 1 shows cephalometric landmarks and planes used in the study of oral cavity and pharyngeal cavity area.
1. Line A-A' was drawn through the most anterior point of the nasal spine of the maxilla (ANS) to the most posterior limit of the nasal spine (PNS). This line, which separates the nasopharynx from the oropharynx, was used as a reference for the other borders of the vocal tract (i.e., oral cavity and oropharynx).
2. For the superior border, lines B-C and C-C' were drawn from the tip of the mandibular central incisor '(B) along the curvature of the incisor alveolar ridge and bony palate, to the most superior aspect of the palatal arch (C). From here a line C-C' parallel to A-A' was drawn through / the posterior pharyngeal wall.
3. The shadow of the posterior pharyngeal used as the posterior border of the vocal
4. For the inferior border, line D-D' was from the most superior point of the body of the hyoid (D) parallel to line A-A' and intersecting the posterior pharyngeal wall at D'. This line separates the oropharynx from the hypopharynx.
5. Line B-B' which indicates the inferior border of the oral cavity, was drawn from point B at the tip of the mandibular central incisor, parallel to line A-A' and passing through the posterior pharyngeal wall at point B'.
6. The anterior pharyngeal border is denoted by line E-A', which was drawn from point E, where line D-D' intersects the shadow of the anterior pharyngeal wall, to point A', the posterior limit of the nasal spine. Line E-A' intersects B-B' at point F and line C-C' at point G.
7. The oral cavity, that area enclosed within lines B-C, C-G, G-F and F-B, is indicated by the shaded area in Fig. l.
8. The pharyngeal area is that part enclosed by lines G-C', C'-D', D'-E, and E-G.
The areas of the oral cavities were then calculated with the use of AUTO CAD software. The pharyngeal cavities were then calculated with the use of a planimeter. This instrument was used to measure the same subject on three different occasions, and the correlation between the scores was reliable according to the formula:
A = M (FR - IR + 10N + C)
Where A = area of figure M = 100, FR = final reading, IR = initial reading, N = the number of times the "0" mark on the centimeter scale is crossed by the pointer, and C = a constant equal to 0 when the anchor point is outside the figure.The mean oral cavity area thus obtained was multiplied with the width between the upper first molars to obtain the oral cavity volume. The mean oral cavity area and the mean pharyngeal cavity area were added, and the resulting sum was multiplied by the width between the upper second molars to obtain the total tract volume (Total tract volume - oral cavity volume = Pharyngeal cavity volume). These oral and pharyngeal cavity volumes of the different groups were then subjected to statistical analysis
Nasopharyngeal dimensions and soft tissue structures (Fig. 2)
In Fig. 2, cephalometric landmarks, planes, and angles were used to study nasopharyngeal dimensions and soft tissue structures.[3]
 | Fig.2. Cephalometric Landmarks, Planes And Angles Used In Study Of Nasopharyngeal Dimensions And Soft Tissue Structures.
|
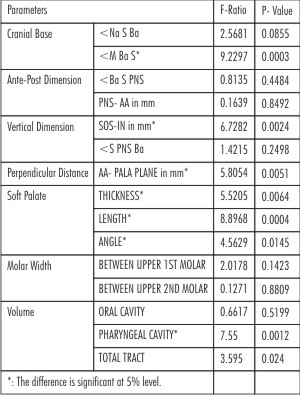 | Table I. Anova For Nasopharyngeal Variables
|
Angulations of the cranial base. A line, M-Ba, was drawn from the posterior border of the foramen magnum (M) to a point on the anterior border of the foramen magnum (Ba) to represent the plane of foramen magnum.
A second line, Ba-S, was drawn from Ba to S, center of sellaturcica. This line represents the basio-sphenoid plane. The angle formed by lines M-Ba and Ba-S (and <M Ba S) represents the posterior angle of the cranial base (1). Next, a line was drawn from the nasion (Na) to sellaturcica to (S).
The angle formed by the intersection of NaSwith SBa (<NaS Ba) represents the anterior angle of cranial base (2).
Anterior-posterior dimension of the pharynx.A line was drawn from point S on the sellaturcica to point PNS on the posterior nasal spine to form an angle with the basiosphenoid plane and express in angular dimension the size of the nasopharynx (<Ba S PNS) (3).
Line PNS-AA represents the linear measurement from point PNS to point AA on the anterior arch of the atlas, or the distance from the posterior nasal spine of the maxilla to the anterior arch of the atlas (I).
Vertical dimension of the nasopharynx.. To establish a basic cranial plane, a line was drawn from Ba toNa. The plane represented by Ba-Na
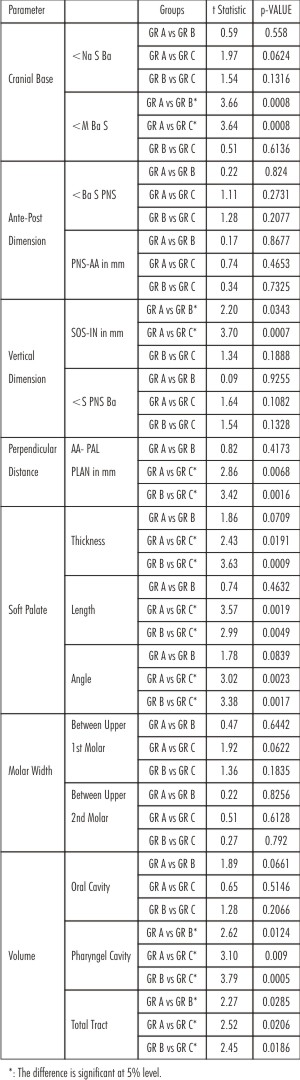 | Table II. Comparative Measurement For Patients With Group A, Group B And Group C Speech
|
was one of the first to used in anthropometry and was observed to extend almost parallel to the roof of the nasopharynx.
To study the superior-inferior dimensions of the nasopharynx, a line was dropped at right angles to the Ba-Na plane from the center of the sphenooccipitalsuture (SOS) to the line PNS-AA. The inferior end of point this line, point IN, represents the inferior extent of the bony nasopharynx of this plane. (ii).
The mean of the angles formed by the points S, Ba, and PNS represented the dimensions of superior and inferior angles of the nasopharynx: LBa S PNS (3), Ba (4), and LPNS Ba S (5).
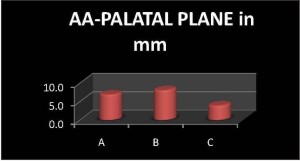
Relation of the palate to the atlas. To determine the of the anterior arch ofthe atlas to the palatal a line was drawn from point PNS to point ANS on the anterior nasal spine and extended posteriorly to the palatal plane.
A line drawn from point AA perpendicular to the palatal plane revealed the position of the anterior arch atlas with respect to the palatal plane (iii).
Soft palate variation. The last group of measurements was designed, first, to find the length and thickness of the soft palate and, second, to determine its angular relationship to the hard palate.
A line was drawn from point PNS to the most inferior point on the soft palate (SP) to represent the length of the soft palate (iv).
A line was drawn from a point midway on the postero-inferior surface to a corresponding point on the antero-inferior aspect of the soft palate to represent the thickness of the soft palate.
The angle formed at the junction of ANS-PNS and PNS-S (with S being a point on the inferior curvature of the soft palate) represented the angle of the soft palate.
Three readings of each linear measurement and angle were obtained for each patient and the means were calculated. The obtained data were subjected to statistical analysis in which the arithmetic mean and the standard deviation of the variables of each group werecalculated and then subjected to Student'st test for unpaired data to obtain the significance. Data were also subjectedto the analysis of variance test.
Result
Mean, standard deviation, student t-test and ANOVAstastical test were done for this study using Epi info software.The present study shows that there is a significant change in the posterior cranial base angle between persons with repaired cleft palate patient and patients with unrepaired cleft palate, both are known to have speech disorders (Table 1). The posterior cranial base angle is much greater in the case of repaired cleft palate. Increases in total tract volume and pharyngeal cavity volumes also were found in persons with repaired cleft palate when compared with patients with normal nasopharyngeal construction and patients with unrepaired cleft palate. (Table 2).
The soft palate was found to be significantly reduced in thickness and length, with a decreased angle in repaired and unrepaired cleft palate patient compared with that of patients with normal speech. The only difference in the hard and soft structures between patients with repaired cleft palate speech and those with normal speech was that the posterior cranial base angle and the pharyngeal cavity and total tract volume were both slightly decreased in the former, with a significant shortening of the soft palate.
The results are presented graphically in Fig.3 through 10
Discussion
The nasopharyngeal area in man is one of great complexity, involving as it does structures that are intimately concerned with the important functions of mastication, swallowing, respiration, olfaction, and speech.
Important through the entire area are numerous controversial opinions regarding the comparative size of the nasopharynx is persons with normal palates and those with cleft palates. Kirkham,[24] Wardill,[25] and Psaumes[26] concluded that the lateral dimension of the pharynx is wider in person with cleft palates. Osborne et al[27] have suggested that cervical spine abnormalities cause increased depth and may predispose to velopharyngeal incompetence, which can influence both speech and swallowing; their study also supports the belief that an abnormally wide nasopharynx exists in cleft palate cases.
The only difference in the hard and soft structures between patients with repaired cleft palate Speech and those with normal Speech was that the posterior cranial base angle and the pharyngeal cavity volume were both slightly decreased in the former, with a significant shortening of
 | Fig.3. Differences In Mean Values For Posterior Cranial Angle In Group A, B And C.
|
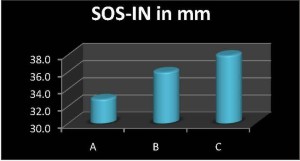 | Fig.4. Differences In Mean Values For Vertical Dimension In Group A, B And C.
|
 | Fig.5. Differences In Mean Values For Perpendicular Distances In Group A, B And C.
|
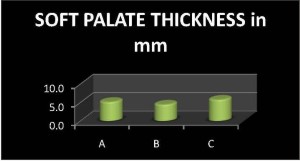 | Fig.6. Differences In Mean Values For Soft Palate Thickness In Group A, B And C.
|
the soft palate; these differences explain the escape of air through the nose during Speech production by repaired cleft palate patients with nasal Speech.
If you consider the normal individual and unrepaired palate patient, the soft palate thickness, length and angle decreased compared to normal and increase in pharyngeal cavity volume and total tract volume in unrepaired palate patients which causes the escape of air both in palate and nose compared to normal Speech.
In unrepaired cleft palate and repaired cleft palate Speech have hyper nasality but the unrepaired have problem in palatal sound compared to repaired cleft palate patient.
Conclusion
It can be concluded from the obtained data that there is an increase in the width and depth ofthe nasopharynx, with a consequential increase in pharyngeal cavity volume and total tract volume in patients who have repaired cleft palate speech compared with that of patients who have normal speech and those who have unrepaired cleft palate speech.
The thickness, length, and angle of the soft palate are all decreased in persons with repaired and unrepaired cleft palate when compared with those of persons with normal speech. There is also a decrease in the depth of the nasopharynx and the length of the soft palate in persons with repaired cleft palate speech, compared with those with normal speech.
These variations in anatomic structures are major contributors to deviations in voice quality and articulation. So lateral cephalometry may be the initial diagnostic criteria for speech disorders cleft lip and palate patients.
So lateral cephalogram can be used as an initial diagnostic criterion for speech disorders.
References
1. Proffit WR and McGlove RE. Correlation between functional lingual pressure and oral cavity size. Cleft palate J 1972;9:229-35
2. Proffit WR and McGlove RE. Lip and tongue pressures related to dental arch and oral cavity size in Australian aborigines. J Dent Res 1975;54:14-47
3. Ricketts RM cranial base and soft structures in cleft palate speech and breathing. PlastReconstru SUR 1954;14;47
4. Calnan J. Diagnosis prognosis and treatment of palatopharyngealicompetence with special reference to radiographic investigation. Br J PlastSurg 1956;8:256
5. Russel GO. The vowel: its physiological mechanism as shown by X-ray. Columbus: ohio state university press, 1928(as quoted in a cineflurographic study of palatal incompetency cases)
6. Russel GO. The mechanism of speech. J AcoustSoc Am 1929;1:83
7. Paramenter CE vowel position as shown by X-ray. Q J Speech 1932;18:351
8. Mcmillan and Keleman C radiographiy of the supraglottic speech organs. A survey. arch Otolaryngol 1952;55:671
9. Subtelney JD application of roentigenegraphy in study of speech. Mannusals of phonetics, 1957.
10. Broadbent RH a new x-ray technique and application to orthodontics. Angle othodo 1931;1:45
11. Subtelny JD. Width of nasopharynx and related structures in normal and unoperated cleft palate children. Am J Ortho 1955;41:889
12. S A Jakhi and F R Karjodkar . Use of cephalometry in diagnosing resonance disorders. Am J DentofacOrthop 1990;98:323-32
13. Subtelny JD. laminography study of vowels produced by cleft speaker. Chicago, illinosis:northwesyern university, PhD dissertation, 1956
14. Carrel J. A cineflourographic technique for the study of velo-pharyngeal closure. JSpeech Hear Disord 1952;12:224
15. Ysunza A, Pamplona C, Toledo E. Change in velopharyngealvalving after speech therapy in cleft palate patients. A videonasopharyngoscopic and multi-view videofluoroscopic study. Int JPediatrOtorhinolaryngol. 1992 Jul;24(1):45-54
16. Fujimura o. computer controlled radiography for observation of movements of articulatory and other human organs. Comput Biomed 1973;3:371-84
17. Sawashima m. current instrumen tation and technique for observing speech organs. Techocra 1976; 9:19-26.
18. Casal C, Domínguez C, Fernández A, Sarget R, Martínez-Celdrán E, Sentís-Vilalta J, Gay-Escoda C. Spectrographic measures of the speech of young children with cleft lip and cleft palate. Folia PhoniatrLogop. 2002 Sep-Oct;54(5):247-57.
19. Tachimura T, Nohara K, Fujita Y, Wada T. Change in levatorvelipalatini muscle activity for patients with cleft palate in association with placement of a speech-aid prosthesis. Cleft Palate Craniofac J. 2002 Sep;39(5):503-8
20. Ueda N, Sato Y, Senoo Y, Mori T, Moriguchi T, Nakagawa H. New design of a palatal lift prosthesis combined with a palatal bar. Cleft Palate Craniofac J. 2002 Jan;39(1):12-7
21. Ysunza A, Pamplona MC, Molina F, Drucker M, Felemovicius J, Ramírez E, Patiño C. Surgery for speech in cleft palate patients. Int J PediatrOtorhinolaryngol. 2004 Dec;68(12):1499-505
22. Pruzansky S. Role of orthodontists in cleft palate. PlastReconstSurg 1954;14:10
23. Kirkham HLD. Measurement of palates at various ages cited in subtenny JD width of the nasopharyn and related anatomic structures in normal and unoperated cleft palte children. Am J Orthod 1955;41:889
24. Wardill WEM. Cleft palate. Br J Surg 1928; 76:127.
25. Psaume J. Description, classification and analysis of unoperated cleft of the lip and palate. Am J Orthod 1953; 39; 590-611.
26. Osborne GS. Upper cervical spine anomalies and nasopharyngeal depth. J S peech Hear Res 1971; 14:141. |