INTRODUCTION
Most difficult and common problem which is described and analyzed by many orthodontists is Gagging or retching which has been found extremely difficult to treat. A wide range of strategies is presented to aid the clinician with the treatment of these patients. Pharyngeal reflex is a normal involuntary defense mechanism that prevents foreign bodies from entering the trachea, pharynx or larynx(1). Unwanted, irritating or toxic material is ejected from the upper respiratory tract by the contraction of oropharyngeal muscle. In retching peristalsis become spasmodic, uncoordinated and the direction is reversed. Gag reflex is also caused when soft palate or posterior pharynx or soft palate is touched, which is the most common reason for gagging during impression making. Patient may present with wide variety of symptoms like excessive salivation, lacrimation, coughing, fainting or in minority of patients, a panic attack and sweating , at times a full-body response may occur. The patient may extends the head, arms, neck and back in an attempt to completely withdraw from the offending stimuli. The patient may have wide range of disruptive reaction; from simple contraction of palatal or circumoral musculature to spasm of the pharyngeal structures, accompanied by vomiting(2,3,4).
after insertion of the denture and may be due to an
DISCUSSION:
Gagging may be elicited by non tactile and tactile stimulation of certain intraoral structures. Five intraoral areas is known as trigger zones:
• palatoglossus & palatopharyngeal folds,
• base of tongue palate,
• uvula and
• Posterior pharyngeal wall.
Nontactile sensations such as-visual, auditory, olfactory stimuli.
Etiology of gagging-
Various etiological factors of gag reflex are Local and systemic disorders, Anatomic factors ,Psychological factors, Physiologic factors, Iatrogenic factors
Management Clinical techniques-
1. Teaching the patient to swallow with their mouth open- It has been suggested that all patient who gag characteristically swallow with their teeth clenched, using the teeth, lips and cheeks as a buttress for the tongue to push against. Teaching the patient to swallow with teeth apart, the tip of the tongue placed anteriorly on the hard palate, and orbicularis oris relaxed, has been advocated.
PSYCHOLOGICAL TECHNIQUE-
1. Behavior modification- it is the most successful long term method of managing the gagging patient. Generally the objective is to reduce anxiety and unlearn the behavior that provokes gagging. Relaxation, distraction, suggestion and systemic desensitization.
• Relaxation-ask the patient to tense and relax certain muscle groups, starting with the legs and working upwards, while continually providing reassurance in a calm atmosphere.
• Distraction- it is useful to temporarily divert a patient attention and may allow a procedure to be performed.
• Conversation
• Concentrate on breathing
• Inhaling through the nose and exhaling through mouth
• Asking the patient to raise legs of the dental chair and hold the position
• Use of a mantra that is repeated silently throughout the procedure may be helpful.
• Sensory flooding- it is accomplished by encouraging the patient keep removable aplliance in mouth as long as possible with the reassurance that the aversive reaction encountered will diminish.
• Cognitive behavioral therapy- changing irrigational thought processes
• Hypnosis
• Praise patient
• Pleasant environment
• Acupuncture-Acupuncture(5) is a system of medicine in which a fine needle is inserted through the skin to a depth of a few millimeters, left in place for a time, sometimes manipulated and then withdrawn. Dental treatment was then carried out and the effectiveness of acupuncture in preventing gagging is assessed.
 |
 |
METHOD
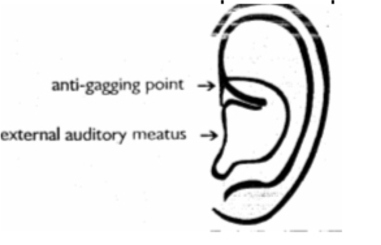
Ear acupuncture was selected for the following reasons:
• There is a specific, recognised anti-gagging point on the ear The needles are not disturbed during access to the mouth for dental treatment
• The needles are Out of the patient’s line of vision — a bonus for anyone with a dislike of needles
• The technique involves the insertion of one, fine, single-use disposable needle of 7mm length into the anti-gagging point of each ear to a depth of 3 mm. The needles are manipulated for 30 seconds prior to carrying out dental treatment. The needles remain in Situ throughout treatment and are removed before the patient is discharged. The patient does not require an escort and is not inconvenienced in anyway following treatment.
The magnitude of the gag reflex was assessed using the gagging severity Index (GSI) prior to acupuncture.
Gagging severity index (GSI)
The gagging reflex is:
I - Very mild, occasional and controlled by the patient
II.-Mild, and control is required by the patient with reassurance from the dental team
Ill.Moderate, consistent and limits treatment options
IV Severe and treatment is impossible
V -Very severe: affecting patient behaviour and dental attendance and making treatment impossible.
The Gagging Prevention Index (GPI) was used to assess the effectiveness of the ear acupuncture in controlling the reflex and allowing dental treatment to take place.
Gagging prevention index (GPI)
Treatment management method employed:
I Obtunded gag reflex; treatment successful
II. Partially controlled gag reflex; all treatment possible
Ill.Partially controlled gag reflex but frequent gagging; simple treat- mere possible
IV. Inadequately controlled gag reflex; simple treatment unable to be completed
V Gag reflex severe; no treatment possible.
On the completion of treatment, the needles were removed. All acupuncture treatments were carried out by one dentist trained in dental acupuncture.
MECHANISMS OF ACTION
The neurophysiology of acupuncture analgesia is well explained while that of ear acupuncture in controlling the gag reflex is not. Indeed the traditional explanation of ear acupuncture is at odds with any scientific basis. The ear correspond with the area of skin of the external auditory meatus innervated by the auricular- branch of the vagus nerve, and is adjacent to an area innervated by the auriculo-temporal branch of the mandibular division of the trigeminal nerve. The vagus nerve is related to swallowing and gagging. Between them, the vagus and the trigeminal nerves are responsible for much of the sensory innervation of the laryngeal, pharyngeal, palatal and oral musosa, and the motor inervation of the musculature of the larynx, pharynx and palate.
PLACEBO EFFECT
The placebo or suggestive effect of treatment can be very powerful. A recent systematic review has confirmed that the placebo effect is mediated via endogenous opioids.
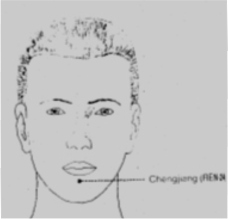
Acupressure- follows the same principle as acupuncture, but the former stimulate’ the points with gentle finger pressure rather than fine needles and therefore is a less invasive technique. Chengjiang (REN-24) is an effective acupressure point for controlling the gag reflex during impression making. To make use of it locate the REN—24 point. It is situated in the horizontal mentolabial groove. Approximately midway between the chin and the lower lip. Apply light finger pressure with the index finger progressively increase the finger pressure until the patient feels discomfort and distension. The acupressure should start at least 5 min before impression making, continue through the impression procedure, and be terminated only after the impression has been removed from the patients mouth. Pressure can he applied by the patient, dental assistant, or dentist.
 |
|
• The P-6 Neikuan acupuncture point, located on the wrist, has been used in the Far East for thousands of years for its anti-nausea and anti-anxiety properties. Stimulation is documented in this article. The P-6 point has remarkable anti-gagging effects if stimulation is applied correctly. Clinicians may apply thumb pressure at the P-6 point to achieve some effect, although this is not as effective as acupuncture. Nevertheless, a substantial percentage of gagging patients would be able to go through dental procedures without gagging when the P-6 point is stimulated.
PHARMACOLOGICAL MANAGEMENT-
1. Locally acting- peripher1ily acting drugs/ local anesthesia . They may applied in the form of sprays, gels or lozenges or by injection. The effectiveness of these agents is limited.When mucosal surface is desensitized, the patient is less likely to gag(6). The deposition of LA around the posterior palatine foramen has been used for patient who gags. However, the administration of a local injection may not be possible and may itself provoke gagging. Further more injection of LA solution may distend the tissue resulting in an inaccurate impression, which may compromise retention of prosthesis.
2. Centrally acting drug- it is only a short term solution for severe gagging problem and should not be used routinely
a. Tranquilizers like chlorpromazine are useful in patient under strain/tension 25-100mg
b. Semi hypnotic, antihistamines, parasympatholytics.
Only one clinical evaluation of a drug – Tigan as an- antigagging agent was found in the dental literature. Prior research on this drug indicated successful relief of nausea and vomiting in a number of conditions including pregnancy, motion sickness (7).
Tips for Dentists and Patients: Handling the Gag Reflex
• Gagging can be caused by fear, allow the patient to address his fear to you and your staff members in order to overcome it."
• " Use of table salt on the tip of the tongue. Works 95% of the time.”
• Reassurance-Dentist must reassure the patient that he or she will stop immediately if patient want them to, whether it be to rinse, or just to catch his breath. If we have a trusting relationship, then patient’s sense of control will increase.
• Sitting up rather than lying down can also help with the gag reflex
• Using super-fast setting impression material and letting the patient walk around while the mold is setting also help
• Listening to music
• Situations that have triggered gagging in the past should be avoided
• Providing treatment in short increments can also help.
• Desensitization methods can also work well. Give patients various dental tools such as a mouth mirror and small impression trays. They can then take these home and introduce these instruments into their mouths themselves. They should keep a diary of how long they feel comfortable by timing it. Doing this a few times in a row twice a day, you will become less sensitive to the gag reflex. As a dentist, you can ask the person to practice until, for example, they feel comfortable sitting with the tray in place for 5 minutes.”
• Lift one foot up in the air to have them concentrate on that."
CONCLUSIONS
These are various methods of management of gag reflex .and causes of gag reflex..If dentist is effectively able to control and avoid gag reflex in patient it will lead to efficient dental treatment and hold over patient.
BIBLIOGRAPHY
1.Newton AV The Psycosomatic component in prosthodontics.J Prosthet Dent,1984:52:871-874.
2.Bray JJ.Grag PA. Macknight AD. Mills RG. Taylor DW Lecture notes on Human Physiology. 3rd edition. Bakewell Scientific Publication.1994:Pp:556.
3. Guyton C Hall J Text Book of Medical Physiology. 9th Ed.: W.B. Saunders Company.1996:Pp:849-850.
4. Bassi GS. Humphris GM,Longman Lp The etiology and management of gaging: A Review of literature. J Prosthet Dent,2004;7(2):14-17.
5. Fiske J. Dickinson C The Role of Acupunture in controlling the gag reflex using a review of ten cases. Br Dent J,2001 :190(11):611-613.
6. Linton et al. Rapid elimination of hyperactive reflex. JPD.1988;60(4); 415-417.
7. Kovats JJ. Clinical evaluation of the gagging patient. JPD. 1971; 25 (6);60. |