Introduction
Tooth agenesis is the most prevalent craniofacial congenital malformation in humans. Up to 25% of the population may have a missing third molar. Agenesis of other permanent teeth, excluding third molars, ranges from 1.6 to 9.6%, depending on the population studied. Primary dentition may also be affected, but with lower prevalence (from 0.5 to 0.9%) (Vastardis, 2000)[1]. The majority of persons with hypodontia (80%) lack only one or two teeth, permanent second premolars and upper lateral incisors being predominantly affected (Symons et al, 1993)[2]. However, about 1% (0.08-1.1%) of the population suffers from oligodontia-the agenesis of more than 6 teeth (Stockton et al, 2000[3]; Gabris et al, 2001[4]). Loss of all teeth is known as anodontia. How tooth loss comes about is thus an important question.
Case Report
These are the series of cases which reported to the Department of Pediatric and Preventive Dentistry, ITS Dental College, Muradnagar.
The child was born to nonconsanguineous parents. The pregnancy and delivery were uneventful. There was no history of any severe systemic diseases, any history of trauma, or infections to the anterior region. Family history revealed no such finding in any members of the family.
Case 1: A 3 year old boy presented with a chief complaint of decayed teeth. On intraoral examination lower primary lateral incisors were bilaterally absent. Panaromic examination confirmed bilateral agenesis of deciduous mandibular lateral incisors (Figure 1, Figure 2).
 | Figure 1: Intraoral photograph showing bilaterally missing lateral incisors
 |
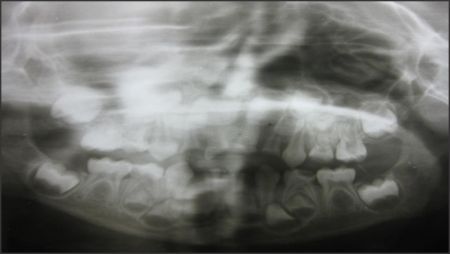 | Figure 2: Panoramic radiograph showing the missing teeth (primary dentition)
|
 | Figure 3: panoramic radiograph showing missing teeth (permanent dentition)
|
Case 2: A 15 year old girl presented with a chief complaint of dirty teeth. Intraoral examination revealed presence of a number of retained deciduous teeth. Henceforth panaromic examination was done to view the status of permanent teeth. OPG of the patient revealed the congenital absence of upper lateral incisors, canines, 1st and 2nd premolars bilaterally. In the lower arch second premolars were found missing bilaterally (Figure 3).
Case 3: A 14 year old boy presented with a chief complaint of forwardly placed upper anterior teeth. On examination lower lateral incisors and second premolars were missing bilaterally. To confirm the diagnosis OPG was taken which substantiated the finding of congenital bilateral absence of lower lateral incisors and second premolars.
Case 4: A 11 year old girl presented with chief complaint of spacing in lower front tooth. On clinical intraoral examination congenital absence of lower lateral incisors was suspected. Patient gave no history of trauma or avulsion of teeth. OPG was taken which confirmed agenesis of mandibular lateral incisors bilaterally.
Case 5: A 14 year old girl presented with a chief complaint of dirty teeth. Intraoral examination revealed extrinsic stains in all teeth. The central incisors were not present bilaterally. Patient gave no history of trauma. IOPA and OPG were taken which confirmed the clinical finding.
Case 6: A 12 year old boy presented with a chief complaint of decayed lower left and right posterior teeth. IOPA and OPG of the patient revealed bilaterally absent second premolars in the lower arch and their was no sign of any presence of crypt formation.
Case 7: A 11 year old girl presented with a chief complaint of pain in lower left back tooth region. Intraoral examination revealed decayed lower first permanent molar and deciduous primary second molar on both the sides. IOPA and OPG of the patient were taken that suggested the absence of right second premolar while a crypt was appreciated of the left second premolar.
Discussion
There appears to be a multifactorial aetiology to hypodontia, with both genetic and environmental factors playing important roles. The pathogenesis of hypodontia cannot be explained by genetic factors alone since monozygotic twins show discordant expression at a certain frequency with respect to hypodontia. Hypodontia is thought to involve environmental factors including infections e.g. Rubella, drugs such as thalidomide and irradiation as well as the developmental relationships between the nerves, maxilla, mandible, oral mucosa, supporting tissues and hard tissues.
Attempts were made to explain them with evolutionary and anatomic models such as Butler's field theory, odontogenic polarity, or Sofaer's model of compensatory tooth size interactions.
According to Butler's theory (1939), mammalian dentition can be divided into 3 morphologic fields corresponding to incisors, canines, and premolars/molars. Within each field, one "key" tooth is presumed to be stable; flanking teeth within the field become progressively less stable. Based on Butler's theory, the third molar and the first premolar would be predicted to be most variable in size and shape.
Clayton hypothesized that the teeth most often missing were "vestigial organs" with little practical value for modern man. In the evolutionary process, these teeth provide no selective advantage for the species and hence have been lost.
Sofaer et al speculated that agenesis occurs when there is insufficient primordia for tooth germ initiation.
Kjaer has explained the location of tooth agenesis by neural developmental fields in the jaws (incisor field, canine/premolar, and molar field). The region within a single field where innervation occurs last is more likely to manifest tooth agenesis.
In the majority of cases, hypodontia has a genetic basis. To date, the mutation spectra of non-syndromic tooth agenesis in humans have revealed defects in two such genes that encode transcription factors, MSX1 and PAX9. Both Msx1 and Pax9 interact during the tooth-bud-to-cap transition. In the mouse, in the absence of either Msx1 or Pax9, tooth development is arrested at the bud stage. The mode of inheritance of MSX1-caused hypodontia is predominantly autosomal-dominant, (Kim et al, 2006)[5]. PAX9 has been found to be the gene causing isolated molar oligodontia, an autosomal-dominant disorder with agenesis of most permanent molars, sometimes in combination with other types of teeth.
Beyond these genetic disorders, tooth loss is triggered by a variety of oral diseases, such as periodontitis and dental caries, and by traumatic and age-related alterations. Hypodontia does not represent a life threatening condition; however, it is connected with masticatory, speech, and esthetic problems.
Clinical Treatment Of Tooth Agenesis
Multiple treatment options are currently available for persons with tooth agenesis. Synthetic dental implants are a widespread standard procedure to replace missing teeth, and its success has increased in recent decades. Different fixtures-such as implant, crown, bridge, fixed or removable, complete and partial dentures-have been shown to be sufficient over the long term (Bartlett, 2007)[6]. The negative outcomes include possible infection causing failure of the implant to integrate with the bone, resulting in implant loss and possible bone loss (Callan, 2007)[7]. Implants placed into developing alveolar ridges have been shown to inhibit ridge formation.
Tooth Engineering: A New Target In Tooth Loss Therapy
The re-organization of tissues in scaffolds to form new tissues/organs is one recent approach. This technique was successfully applied in periodontal regeneration (Duailibi et al, 2004[8]) and has been tested in tooth engineering. So far, embryonic cells from fetuses have been used to form a new tooth de novo. The experiments support mammalian cell plasticity and suggest the existence of a cell-specific developmental program, even after tissue dissociation and growth in culture conditions.
However, much more attractive is the challenge to form a mineralized tooth without any scaffold. Tooth germs can develop successfully following dissociation and re-association without a scaffold support (Hu et al, 2006[9]). This technique would enable one to collect an individual´s cells from any stem cell niche, grow these in the culture, induce them to progress along a tooth-developmental pathway, and create a de novo tooth. Great steps have already been made in this direction, a tooth having been created where the mesenchymal parts were stem-cell-derived (Ohazama et al, 2004[10]). Therefore, the only non-stem-cell-derived parts of the resulting tooth crown were the ameloblasts.
Conclusion
With the increase in prevalence of hypodontia observed over the 20th century, the identification of its causative factors is essential for providing treatment to those afflicted in the future. Modern molecular genetic techniques have allowed us to start to identify the genetic factors responsible for tooth agenesis but more work is required to discover how malfunction in these factors disrupt tooth development. To achieve this, dental professionals need to collaborate with human geneticists for investigative research to increase the known population of mutations affecting the dentition.
References
1. Vastardis. The genetics of human tooth agenesis: New discoveries forunderstanding dental anomalies. American Journal of Orthodontics and Dentofacial Orthopedics2000; 117(6): 650-6
2. Symons AL, Stritzel F, Stamation J (1993). Anomalies associated with hypodontia of the permanent lateral incisor and second premolar. J Clin Pediatr Dent 17:109-111.
3. Stockton DW, Das P, Goldenberg M, D'Souza RN, Patel PI. Mutation of PAX9 is associated with oligodontia. Nat Genet 2000; 24:18-19.
4. Gabris K, Tarjan I, Csiki P, Konrad F, Szadeczky B, Rozsa N. [Prevalence of congenital hypodontia in the permanent dentition and its treatment.] Fogorv Sz 2001; 94:137-140 (article in Hungarian).
5. Kim JW, Simmer JP, Lin BP, Hu JC. Novel MSX1 frameshift causes autosomal-dominant oligodontia. J Dent Res 2006; 85:267-271.
6. Bartlett D. Implants for life? A critical review of implant-supported restorations. J Dent 2007; 35:768-772.
7. Callan DP. Dental implant design and oral and systemic health. Compend Contin Educ Dent 2007; 28:482-492.
8. Duailibi MT, Duailibi SE, Young CS, Bartlett JD, Vacanti JP, Yelick PC. Bioengineered teeth from cultured rat tooth bud cells. J Dent Res 2004; 83:523-528
9. Hu B, Nadiri A, Kuchler-Bopp S, Perrin-Schmitt F, Peters H, Lesot H. Tissue engineering of tooth crown, root, and periodontium. Tissue Eng 2006; 12:2069-2075.
10. Ohazama A, Modino SA, Miletich I, Sharpe PT. Stem-cell-based tissue engineering of murine teeth. J Dent Res 2004; 83:518-522. |