Introduction
Internal resorption is a clinical term used to describe a relatively uncommon, insidious, and often aggressive form of resorption .It is characterized by an oval-shaped enlargement of root canal space (Well demarcated ballooning area). Lesion appears close to the canal even if angulations of radiographs changes. Outline of the canal is distorted. Pink spot is present. Internal resorption may extend to the external surface leading to primary endodontic and secondary periodontal lesion. Internal root resorption leading to communication between pulp space & periodontal ligament produces a complicated situation and a challenge to the clinician for its management. The most recent and promising material used to seal this communication is Mineral Trioxide Aggregate (MTA). It is seen in most cases as a late complication of traumatic injuries of the teeth, but it may also occur after orthodontic movement, orthognatic and other dentoalveolar surgery, periodontal treatment, bleaching of teeth, and a wide variety of traumatic conditions. Mineral trioxide aggregate or MTA (MTA; Pro-Root®, Dentsply Tulsa, Tulsa) is reported to show good sealing ability, a high degree of biocompatibility, and potential to be repair material for internal resoption. In this case report, the internal resoption was repaired with MTA and the rest of the canal was filled with gutta percha points.
Case Report
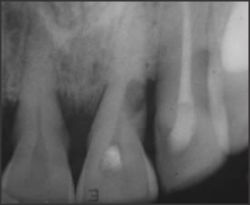
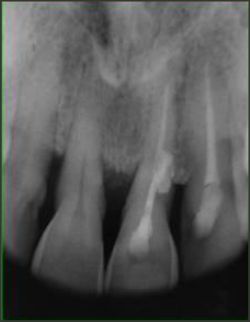
A 44-year-old male patient presented with a complaint of acute pain in upper left front teeth region that started a month before reporting (picture 1). Patient had a history of trauma 6 months back. His medical history was noncontributory. On the clinical examination of the anterior maxillary region, it was noted that the maxillary central incisor was painful during biting and percussion. The tooth was unresponsive to sensitivity testing with cold or an electric pulp tester (Parkell, Farmingdale, NY, USA). Radiographic examination demonstrated an apparent radiolucency in the middle third of the root canal (picture 2). There was clinically obvious pinkish color in tooth especially on the lingual side. There was bleeding sign on probing and recession of 3mm distobuccally, 2mm bucally and 2mm mesiobucally was calculated (picture 3). Clinical and radiographic examination indicated pulp necrosis with resorption causing lingual perforation. Grade II mobility was present. The patient was given a detailed explanation concerning the planned treatment procedure and prognosis. The tooth anesthetized followed by a conventional access cavity preparation and the cavities were widened with an Endo-Z bur (Dentsply Maillefer, Tulsa, OK) to enhance the visibility of the root canal. Irrigation of the canal was done several times with 5% sodium hypochlorite, and the last irrigation solution was left in the canal for 15 minutes to dissolve organic material. The canal was filled with calcium hydroxide, cotton and zinc oxide eugenol. At the next visit, determination of the working length was done using an electronic apex locator
 | Picture 1
 |
 | Picture 2
|
 | Picture 3
|
 | Picture 4
|
 | Picture 5
|
 | Picture 6
|
 | Picture 7
|
(Root ZX, J Morita Corporation. Kyoto, Japan). Canal enlargement was done with hand k-files. At the third visit, which was one week after initial visit, local anesthesia was administered, and mucoperiosteal flap was raised (picture 4)
 | Picture 8
|
 | Picture 9
|
 | Picture 10
|
 | Picture 11
|
and the lesion was exposed (picture 5). Lesion on the root surface was located with a periodontal probe as shown in picture 6. A 15no k-file is shown passing through the access opening to the external surface of the lesion (picture 7). MTA was mixed with sterile water to a paste consistency following the manufacturer's instructions. MTA was then applied into the resorption defect with a small sized plastic filling instrument (picture 8). The remaining root canal was filled with gutta-percha points and sealer (AH26, Dentsplay, Konstanz, Germany) using a lateral condensation technique. Bone graft material hydroxyappatite crystals were applied on the MTA filled resorption lesion over the root surface (picture 9).A gingival tissue regeneration membrane was then placed (picture10) and the flap was then sutured (picture 11). A periodontal pack was placed on the sutured gingival (picture 12). The patient was recalled after 8-9 days, the pack was removed and sutures were removed. On clinical examination mobility reduced but recession increased to 4 mm (picture 13). Patient was regularly examined at an interval of 1 month (picture 14), 6 months, and then 1 year follow up radiographically. (picture 15).
Discussion
MTA has an excellent sealing ability in the presence of moisture in a root canal. This property is especially important in teeth with perforation and resorption because the material may be exposed to oral fluids. Local anesthesia was administered because the operator wanted to relieve the pain that the patient may experience when the filling material was packed against the tissue. The surgical intervention of perforation and resorption repair with MTA were reported to be successful. Formation of a physiological gingival crevice, function regeneration and maturation of the gingival connective tissue requires 3 to 5 weeks and surgical intervention would be more difficult if the defect was located on the lingual aspect of the root. In this case, 5% sodium hypochlorite was left in the canal for 15 minutes to dissolve the tissue. Sodium hypochlorite is well known to be effective in removing the smear layer from the canal walls and reducing the microorganisms and inflammatory reaction with its availability in the clinic. Both clinical and radiographic follow-up showed a stable
 | Picture 12
|
 | Picture 13
|
 | Picture 14
|
 | Picture 15
|
condition without any probing defect, ongoing root resorption, or apical pathosis. MTA causes formation of cemetal layer over the sealed area. MTA preferentially induced alkaline phosphatase expression and activity in both periodontal ligament and gingival fibroblast. It helps in the bone regeneration adjacent to sealed area. Most of the cell studies showed good cell growth over MTA with the formation of a cell monolayer over the material. MTA allows overgrowth of cementum & periodontal ligament . Presence of cementum on the surface of MTA was a frequent finding. MTA actively promotes hard tissue formation rather than being inert or an irritant. The condensation of fibronectin around the formed apatite crystals permits cellular adhesion and differentiation seen as cementoblast in the periodontium. MTA supported almost complete regeneration of the periradicular periodontium. MTA had antibacterial effects against facultative anaerobes but not agianst obligate anaerobes. Osteocalcin levels were also increased in the presence of MTA. MTA (ProRoot) also preferentially induced alkaline phosphatase expression and activity in both periodontal ligament and gingival fibroblast. To this case report confirms that the pocket depth in the resorption area sealed with MTA was reduced due to regeneration of cementum, periodontal ligaments as well as bone over the resorption area. MTA is the ideal material for repair of resorption lesions especially the internal resortion extending to the outer surface of the root leading to Endo-perio lesion.
References:
1. Heithersay GS. Invasive cervical resorption: an analysis of potential predisposing factors. Quintessence Int. 1999 Feb;30(2):83-95.
2. Gonzales JR, Rodekirchen H. Endodontic and periodontal treatment of an external cervical resorption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 Jul;104(1):e70-7.
3. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod. 1993 Dec;19(12):591-5.
4. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod. 1993 Nov;19(11):541-4.
5. Arens DE, Torabinejad M. Repair of furcal perforations with mineral trioxide aggregate: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996 Jul;82(1):84-8.
6. Baratto-Filho F, Limongi O, Araújo Cde J, Neto MD, Maia SM, Santana D. Treatment of invasive cervical resorption with MTA: case report. Aust Endod J. 2005 Aug;31(2):76-80.
7. Pace R, Giuliani V, Pini Prato L, Baccetti T, Pagavino G. Apical plug technique using mineral trioxide aggregate: results from a case series. Int Endod J. 2007 Jun;40(6):478-84.
8. Hsien HC, Cheng YA, Lee YL, Lan WH, Lin CP. Repair of perforating internal resorption with mineral trioxide aggregate: a case report. J Endod. 2003 Aug;29(8):538-9.
9. Ford HE, Ford TR. Surgical repair of a resorptive defect in an anterior tooth of an adolescent: a case report. Int J Paediatr Dent. 1998 Sep;8(3):219-22.
10. Ramfjord SP, Engler WO, Hiniker JJ. A radioautographic study of healing following simple gingivectomy. II. The connective tissue. J Periodontol. 1966 May-Jun;37(3):179-89.
11. Hunt PR. Safety aspects of mandibular lingual surgery. J Periodontol. 1976 Apr;47(4):224-9.
12. Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int. 1999 Feb;30(2):96-110.
13. Teixeira CS, Felippe MC, Felippe WT. The effect of application time of EDTA and NaOCl on intracanal smear layer removal: an SEM analysis. Int Endod J. 2005 May;38(5):285-90.
14. Jiménez-Rubio A, Segura JJ, Llamas R, Jiménez-Planas A, Guerrero JM, Calvo JR. In vitro study of the effect of sodium hypochlorite and glutaraldehyde on substrate adherence capacity of macrophages. J Endod. 1997 Sep;23(9):562-4.
15. Ercan E, Ozekinci T, Atakul F, Gül K. Antibacterial activity of 2% chlorhexidine gluconate and 5.25% sodium hypochlorite in infected root canal: in vivo study. J Endod. 2004 Feb;30(2):84-7. |