Introduction
Currently, success in endodontic treatment is rated to be as high as 95%. In order to achieve endodontic success it is critical that, the entire root canal system must be debrided, disinfected and obturated [1].
Literature search reveals that the mandibular premolars exhibit highest incidence of variations in root canal anatomy [1]. Hence, additional root canals must be detected in all cases otherwise treatment failure is extremely possible [2],[3],[4].
Variations in root canal morphology reportedly occur more frequently in mandibular first premolars than in the second premolars [5],[6],[7]. Racial differences in root canal morphology of these teeth has also been well established [6],[8].
A study conducted by Cleghorn et al[9] reported that 98% of mandibular first premolars had a single root, 1.8% had two roots, and 0.2% had three roots. Four roots were extremely rare and were found to be less than 0.1% of teeth studied. Fisher et al[10] and Chang et al have also reported cases of mandibular first premolars with three roots and three root canals. However endodontic management of bilaterally occurring
 | Figure 1
 |
mandibular first premolar with three distinct roots and three separate root canals has never been reported in literature so far.
This case report presents a successful, non-surgical endodontic management of bilaterally occurring three rooted mandibular first premolars.
Case Report
A 38 year old female patient was referred to our department for emergency endodontic management of Tooth # 21 (mandibular left first premolar) and tooth # 28 (mandibular right first premolar) following iatrogenic pulpal exposure during crown preparation. Medical history was non-contributory. Dental history revealed that she had undergone extraction of her lower six anteriors two years back due to non restorable lesions and had now decided to go in for a fixed prosthesis in relation to it. The referring dentist had planned to use teeth # 20, # 21, # 28, # 29 as abutments for the fixed prosthesis and crown preparation was done in relation to them.
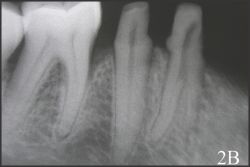
Pre-operative photographs (Fig. 1) and radiographs (Fig. 2A-D) provided by the
 | Figure 2 A
|
 | Figure 2 B
|
 | Figure 2 C
|
 | Figure 2 D
|
 | Figure 3 A
|
 | Figure 3 B
|
referring dentist revealed normal coronal morphology of the tooth # 21 and tooth # 28 but the root canal anatomy of these teeth was quite unusual.
On clinical examination, the patient's oral hygiene was found to be moderate, and lower six anteriors were missing. Crown preparations were observed on tooth # 20, # 21, and tooth # 28, # 29 with pulpal exposure evident on the mesioocclusal aspect of tooth # 21 and # 28.
The involved teeth were tender on percussion. No periodontal pockets were present on either of them and thermal and electrical pulp testing elicited a positive response.
Radiographic evaluation revealed an unusual, bilateral complex root canal anatomy of the tooth # 21 and tooth # 28 (Fig. 2A-D). Vague outlines of the two roots could be identified on the radiographs. Additional radiographs taken at different angulations revealed the presence of an additional root. Crown preparation was also observed in relation to # 20, # 21 (Fig. 2B) and # 28 and # 29 (Fig. 2D) with almost negligible remaining dentin thickness on the mesioocclusal aspect of tooth # 21, # 28 suggestive of a pulpal exposure.
On the basis of the clinical and radiographic findings, a diagnosis of iatrogenic pulpal exposure of tooth # 21 and tooth # 28 was made. Once the confirmatory diagnosis was made, endodontic management of the involved teeth were planned.
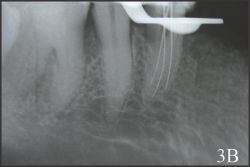
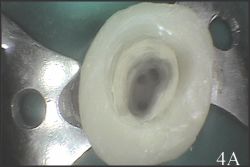
After administration of local anaesthesia, coronal build up of the involved teeth was done with universal composite resin restorative material (3M ESPE Dental Products, St Paul, MN) for application of rubber dam clamps. The teeth were then isolated with rubber dam and the access opening was done keeping in mind the probable location of the orifices of the three root canals. (Fig. 3A and Fig. 4A)
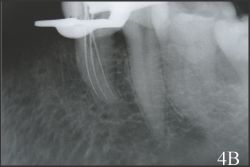
On careful inspection of the pulp chamber floor with the operating microscope, three separate root canal orifices were observed (one mesial, one distobuccal, and one distolingual) both in tooth # 21 and # 28. Coronal flaring for all the three canals was carried out with Gates Glidden drills and working length was determined with the help of apex locator (Root ZX, Morita, Tokyo, Japan), which was later confirmed with a radiograph (Fig. 3B and Fig. 4B).
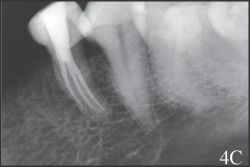
The canals were cleaned and shaped with Protaper (Dentsply, Maillefer, Ballaiques, Switzerland) rotary instruments under copious irrigation with 2.5 % Sodium hypochlorite and 17 % ethylenediaminetetraacetic acid (EDTA). The finishing of canals was performed until Protaper F2 reached the full working length. Root canals were dried with sterile paper points (Dentsply, Maillefer, Ballaiques, Switzerland). Calcium hydroxide paste (Calcicur ; VOCO, Cuxhaven, Germany) was applied and access temporarily sealed with Cavit (3M ESPE AG, Seefeld, Germany). The patient returned after one week. Both teeth were completely asymptomatic. Calcium hydroxide paste was removed and roots canals were obturated by cold lateral compaction of gutta percha using zinc oxide and eugenol (ZOE) sealer (Kemdent, Associated Dental Products Ltd, Wiltshire, UK). A post operative radiograph was taken (Fig. 3C and Fig. 4C) and the access was restored permanently with universal composite resin restorative material (3M ESPE Dental Products, St Paul, MN). One year recall radiographs of both the teeth revealed a healthy periapical bone (Fig. 3D and Fig. 4D).
Discussion
Variations in root canal anatomy of mandibular premolars occur far more often than one can expect. Hess[12], Mueller[13], Amos[14], Ring[15] and Green[16] reported the presence of two canals in 2-17.9% of the teeth studied, with no reports on the presence of three canals.
Pineda and Kuttler[17] reported 0.9% of these teeth with three root canals whereas studies by Zillich and Dowson [5] reported three root canals in 0.4% to 0.5% of the teeth investigated.
Like the number of root canals the number of roots may also vary. Anatomic studies by Cleghorn et al [9] on 4,462 teeth revealed that 97% of mandibular first premolars had only a single root. Two roots were found in 1.8% of the teeth studied. The incidence of three roots was 0.2% and four roots were present in less than 0.1% of the teeth studied. Iyer et al[18] have reported the incidence of three roots as 0.2% and Geider et al[19] reported it to be
 | Figure 3 C
|
 | Figure 3 D
|
 | Figure 4 A
|
 | Figure 4 B
|
 | Figure 4 C
|
 | Figure 4 D
|
2.4%. Four rooted varieties have also been reported, but are less than 0.1%. [9]
Racial differences in root canal morphology have also been reported. The frequency of premolars with two and three root canals appears to be higher in the Asian population[20]
Considering the fact that so much of aberrations exist in these teeth, it becomes mandatory for the clinicians to look for extra canals during the course of endodontic treatment.
Hoen and pink [4] reported 42% incidence of missed roots or canals in these teeth that needed retreatment. A study at the University of Washington which assessed the failure rate of endodontic therapy reported that, the mandibular first premolar had the highest failure rate at 11.45% [1]. Numerous other incidences of failures and flare ups have been reported[1] during endodontic management of these teeth. This could possibly be due to the highly variable and extremely complex root canal anatomy of these teeth.
Radiographs produce only a two dimensional image of a three dimensional object resulting in superimposition of images. Hence, they are of rather limited value in cases with complex root canal anatomy. Interpretation and appraisal based upon a two dimensional radiograph may alert the clinician to the presence of aberrant anatomy but would not be able to confirmatively diagnose the morphological structure of root canals and their interrelations [21].
In such cases the use of operating microscope may be of tremendous advantage in confirming the presence of extra root canals. According to Carr[22] introduction of operating microscope has revolutionised the practice of endodontics. According to Saunders and Saunders[23], by using operating microscope for conventional endodontics, enhanced visualization of root canal intricacies is possible. This would help the clinician to diagnose, clean and shape the entire root canal system more effectively.
A wide range of opinions are reported in literature regarding the number of root canals [9], but there are very few reports on the variations in the numbers of roots [11], [18] that occur in mandibular first premolars. Endodontic management of bilaterally occurring three rooted mandibular first premolars had never been reported in literature so far.
Conclusion
Successful non surgical endodontic management of bilaterally occurring mandibular first premolars with three separate roots and root canals has been presented. To achieve predictable results, thorough debridement of the entire root canal system is imperative. During the course of endodontic treatment, the possibility of extra roots and root canals must be considered especially if the tooth in question is a mandibular premolar. The endodontist should always look for a second, third or even fourth root canal so that the entire root canal system can be debrided and success ensured. Enhanced visualization with the operating microscope must also be considered in the diagnosis and management of these teeth with extremely complex and highly variable root canal anatomy.
References
1. Ingle JI, Bakland LK. Endodontics (2003).5th ed, BC Decker, Inc. Elsevier.
2. Slowey RR (1979);Root canal anatomy: road map to successful endodontics. Dental Clinics of North America 23, 555-73.
3. Weine FS (1995) Non surgical re-treatment of endodontic failures. Compend Cont Educ Dent 16, 326-35.
4. Hoen MM, Pink FE (2002) Contemporary endodontic retreatments: an analysis based on clinical treatment findings. Journal of Endodontics 28, 834-6.
5. Zillich R, Dowson J (1973) Root canal morphology of mandibular first and second premolars. Oral Surgery, Oral Medicine Oral Pathology.36, 738-44.
6. Trope M, Elfenbein L, Tronstad L 1986 Mandibular premolars with more than one root canal in different race groups. Journal of Endodontics 12, 343-5.
7. Vertucci FJ (1978). Root canal morphology of mandibular premolars. Journal of American Dental Association 97, 47-50.
8. Walker RT (1988) Root canal anatomy of mandibular first premolars in a southern Chinese population. Endodontics and Dental Traumatology 4, 226-8
9. Cleghorn BM, Christie WH, Dong CC (2007) The root and root canal morphology of the human mandibular first premolar: A literature review. Journal of Endodontics 33, 509-16
10. Fischer GM, Evans CE (1992) A three-rooted mandibular second premolar. General Dentistry 40, 139-40.
11. Chan K, Yew SC, Chao SY (1992) Mandibular premolar with three root canals- two case reports. International Endodontic Journal 25, 261-4
12. Hess W (1925) The anatomy of the root-canals of the teeth of the permanent dentition, Part 1. New York:William Wood and Co.,
13. Mueller AH (1933) Anatomy of the root canals of the incisors, cuspids, and bicuspids of the permanent teeth. Journal of American Dental Association 20, 1361-8.
14. Amos ER (1955) Incidence of bifurcated root canals in mandibular bicuspids. Journal of American Dental Association 50, 70-1
15. Ring AL (1969) Rontgenologisch-anatomische Untersuchungen zur Mehr-wurzeligkeit von Eckzahnen und Pramolaren. Zahnarztliche Praxis 20, 169-73
16. Green D (1973) Double canals in single roots. Oral Surgery, Oral Medicine Oral Pathology 35, 689-96.
17. Pineda F, Kuttler Y (1972) Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surgery, Oral Medicine Oral Pathology 33, 101-10.
18. Iyer VH, Indira R, Ramachandran S, Srinivasan MR (2006) Anatomic variations in mandibular premolars in Chennai population. Indian Journal of Dental Research 17, 7-10
19. Geider P, Perrin C, Fontaine M (1989) [Endodontic anatomy of lower premolars- apropos of 669 cases]. J Odontol Conserv 11-5
20. De Moor RJ, Calberson FL (2005) Root canal treatment in a mandibular second premolar with three root canals Journal of Endodontics 31, 310-3.
21. Holtzman L (1998). Root canal treatment of mandibular second premolar with four root canals: a case report International Endodontic Journal 31, 364-6.
22. Carr GB (1992). Microscopes in Endodontics. Journal of California Dental Association 20, 55-61
23. Saunders W, Saunders E (1997) Conventional endodontics and the operating microscopes. |