|
|
|
| Dentofacial Orthopedics : Improving Esthetics And Enhancing Mandibular Growth - Using A Functional Appliance |
Tarun Singh Phull 1 , Ankit Gaur 2 , Tarun Sharma 3 , Shishir Singh 4 , Pradeep Raghav 5
1 Senior Lecturer Dept of Orthodontics & Dentofacial Orthopedics - Seema Dental College & Hospital,Uttarakhand
2 Private Practitioner - Gaur Dental Care Mayur Vihar, Phase -II, Patpatganj, New Delhi
3 MDS, Senior Lecturer, Dept. of Orthodontics - Seema Dental College, Rishikesh, Uttarakhand
4 Reader, Dept. of Orthodontics & Dentofacial Orthopedics - Subharti Dental College, Meerut, India
5 Professor & Head, Department Of Orthodontics - Subharti Dental College
|
| Address For Correspondence |
Dr. Tarun Singh Phull, Senior Lecturer,
Dept. of Orthodontics & Dentofacial Orthopedics,
Seema Dental College & Hospital, Virbhadra Road,
Rishikesh,Uttarakhand-249203 , India
E-Mail: drtsp80@gmail.com
Tel: 08979415014. |
| Abstract |
| Management of Class II dysplasias has always been a theme of interest to the orthodontist. Correction of skeletal problems during growth has been a topic of debate and controversy as related to the specialization of dentofacial orthopedics. Keeping the treatment goals and the psychological impact of early treatment in mind, it becomes imperative to correct the underlying discrepancy before or at the time of pubertal growth. Use of removable appliances like Twin-block or bionator helps not only in enhancing the profile but also reducing the list of treatment objectives in the second phase of therapy. A proper patient education for compliance of removable appliance should, therefore, be the first step in treatment. The following clinical case reports the importance and effectiveness of such a removable appliance i.e. Twin-block. |
|
| Keywords |
| mandibular growth, Twin-block, profile. |
|
| Full Text |
Introduction
Diagnosis in dentistry is as important as the treatment and its application at the correct age in dentofacial orthopedics becomes more crucial. Class II malocclusions can manifest in various skeletal and dental configurations. Most Class II patients have a deficiency in the anteroposterior position of the mandible.[1] Several treatment options are available for managing Class II problems, and appliances for improvement of profile along with correction of forces by the facial musculature which have been classified as removable/ fixed myofunctional appliances have been used with great success in patients who are positively motivated for the treatment. Several varieties of functional appliances are currently in use that aim to improve skeletal imbalances. Modulation of maxillary growth along with possible improvement in mandibular growth and position, and changes in dental and muscular relationships are the expected effects of these functional appliances.
Norman Kingsley introduced the "bite-jumping" appliance (1879). The Balter's bionator[2] and Twin-block[3] are two of the popular appliances used today of which the latter has been recommended for 24 hour wear for faster and better results. The dynamax appliance developed in 2003 for the treatment of Class II malocclusion has been shown to be less effective in overjet reduction when compared to the results achieved by using Twin-block.[4] According to the classification by Proffit and Fields, Twin-block is a passive tooth-borne appliance. The Twin-block myofunctional appliance was first described by William Clark.[5]
Diagnosis and Case Selection
An 11 years old boy reported to the Department of Orthodontics and Dentofacial Orthopedics, Subharti Dental College, Meerut with the complaint of forwardly placed upper front teeth. The extra oral findings included a convex profile; incompetent lips with a lip trap and deep mento-labial sulcus. The overbite of 7mm (100%) with a scissors bite in relation to 14, 44 & 24, 34 could be attributed to the retruded mandible. Intra-oral examination revealed a molar relation which according to Angle's classification was Class II; a canine relation of Class II; an overjet of 12 mm (Figs. 1 and 2). The
 | Fig. 1 Pre-treatment Extra-oral photographs
 |
 | Fig. 2 Intra -oral photographs showing molar and canine relation
|
 | Fig.3 Patient with the Appliance
|
 | Fig.4 Comparison of extra-oral features after first phase of orthopedic therapy i.e. after retention phase of removal appliance
|
 | Fig.5 Profile changes by enhancing mandibular growth helps in improvement of smile esthetics
|
 | Fig.6 Intra-oral changes: a leveling of curve of spee in lower arch improved the overbite. The deep bite is to be corrected by intrusion of upper incisors in 2-nd phase (fixed therapy)
|
 | Fig.7 Intra-oral changes: correction of molar, canine relation and overjet correction. Correction of developing scissors bite can be appreciated.
|
overall diagnosis could be classified as Class II div 1 malocclusion.
The presence of a retrognathic mandible, the age of the child with a promising growth potential, a favorable mandibular growth pattern, absence of any dental crowding and a positive Visualized treatment objective (VTO) on bringing the mandible forwards by the patient himself, all indiacted that the extra-oral profile and intra-oral developing problems could be treated preeminently using a myofunctional therapy with a preference to the Twin-block appliance. It has been a proven fact that Twin-block is more efficient than the bionator in preventing forward movement of the maxillary molars.[6]
Treatment plan and progress
Bite Registration
For Class II problems, the proper construction bite was taken and the models were articulated with mandibular protrusion. The mandibular advancement was kept 6mm sagitally with a 4mm of interocclusal clearance in the first premolar region.[7] The interocclusal clearance was increased at the region of deep overbite and bite-blocks were designed to allow the free eruption of the lower molars to reduce the overbite by increasing the lower facial height.
The first phase of active twin-block therapy took almost 11 months due to breakages of the lower block. Deep overbite was reduced by selective trimming of the upper block as recommended. [9]
Results
The ANB value changed from 11 degrees to 5 degrees due to increase of SNB from 69° to 74° (and a very slight decrease in SNA). Y-axis increased from 66° to 69° due to simultaneous effects of growth changes and selective eruption of lower posterior teeth (Fig. 6 to Fig. 10, Table I ). There were dento-alveolar changes other than the skeletal ones observed (Table II). The upper molars had distalized and lower molars mesialized (Fig. 10). The overall changes in facial profile and nose-lips-chin relation could be well appreciated (Fig. 4 and Fig. 5, Table III).
Other relevant cephalometric changes
Changes during the active phase of treatment include the following:
 | Fig.8 Intra-oral occlusal changes
|
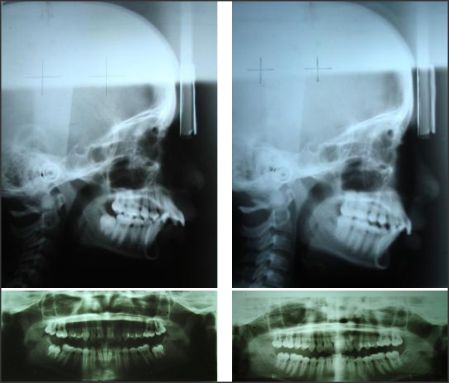 | Fig.9 Comparison of pre - treatment lateral cephalogram and OPG with stage radiographs
|
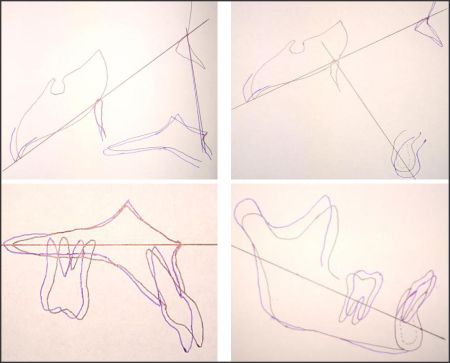 | Fig.10 Ricketts superimposition showing skeletal and dental changes by growth modulation
|
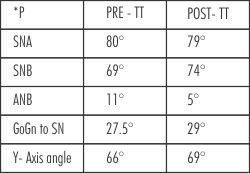 | Table I : Composite Analysis comparing skeletal changes
|
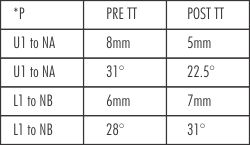 | Table II : Composite Analysis comparing dental changes
|
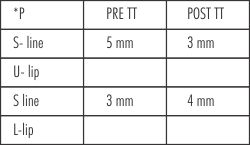 | Table III : Composite Analysis showing soft tissue changes
|
1. Reduction in the anteroposterior apical base discrepancy on angular assessment of ANB angle
2. Increase in effective mandibular length (articulare to gnathion)
3. Increase in facial height (nasion to menton). The majority of patients in the control sample had deep overbite and the aims of treatment were consistent with increasing facial height.
4. Reduction in facial convexity (A point to facial plane)
5. Reduction in the distance from the distal outline of the upper first molar to the pterygoid vertical.
Discussion
In many respects the occlusal inclined plane is a significant improvement on existing appliance mechanisms in the functional guidance of facial growth and development. Significant changes in facial appearances are seen within 2 or 3 months of starting treatment with twin blocks as a result of altered muscle balance and continuous wear, even during eating. Rapid soft-tissue adaptation occurs in response to an improved occlusal relationship.
The most prominent dentoalveolar effect was proclination of the mandibular incisors as a result of the mesial force induced by protrusion of the mandible.
The effect of functional appliance therapy on mandibular growth is a major controversy. Many researchers have claimed that extra mandibular growth occurs with the Twin-block. [8]
Soft-tissue compensation occurs to assist the primary functions of mastication and swallowing, which require an effective anterior oral seal.
The twin block appliance positions the mandible downward and forward, increasing the intermaxillary space. As a result it is difficult to form an anterior oral seal by contact between the tongue and the lower lip, and patients spontaneously adopt a natural lip seal for deglutition without exercises when twin blocks are fitted. [9]
The lip seal is maintained throughout treatment and improved facial balance is evident within a few months of starting treatment.
Conclusion
Orthodontic treatment with the Twin-block functional appliance appears to be effective in correcting molar relationships and reducing overjet in children with Class II div 1 malocclusion. The following conclusions can be drawn:
1. Twin-bock appliance induced mandibular growth by utilization of remaining growth in a child having mixed dentition, therefore, timing of this orthopedic approach was crucial.
2. The appliance was also effective in restricting forward movement of the maxillary molars.
3. The appliance helped dramatically in correction of the molar relationship.
4. Forward movement of the maxillary incisors was restricted.
5. There was an apparent forward movement of the mandibular incisors.
References
1. McNamara JA Jr. Components of Class II malocclusion in children 8-10 years of age. Angle Orthod 1981;51:177-202.
2. Ascher F. The bionator. In: Graber TM, Newmann B, editors. Removable orthodontic appliances. Philadelphia: W. B. Saunders; 1977. p. 229-246.
3. Clark WJ. The Twin-block traction technique. Eur J Orthod 1982;4:129-138.
4. Thiruvenkatachari B, Sandler J, Murray A, Walsh T and O'Brien K. Comparison of Twin-block and Dynamax appliances for the treatment of Class II malocclusion in adolescents: A randomized controlled trial. Am J Orthod Dentofacial Orthop 2010;138:144-145.
5. Clark WJ. The Twin Block technique: a functional orthopedic appliance system. Am J Orthod Dentofacial Orthop 1988; 93:1-18.
6. Jena AK, Duggal R and Prakash H. Skeletal and dentoalveolar effects of Twin-block and bionator appliances in the treatment of Class II malocclusion: A comparative study. Am J Orthod Dentofacial Orthop 2006;130:594-602.
7. De Vicenzo .O. J.P. & Winn. M.W. Orthopaedic and orthodontic effects resulting from the use of functional appliance with different amounts of protrusive activations. Am J Orthod Dentofacial Orthop 1989; 96: 181- 190 .
8. O'Brien K, Wright J, Conboy F, Chadwick S et al. Effectiveness of early orthodontic treatment with the twin-block appliance: a multicenter, randomized, controlled trial Part I: dental and skeletal effects. Am J Orthod Dentofacial Orthop 2003;124:234-243.
9. Clark WJ. Twin block functional therapy. London: Mosby-Wolfe; 1995. |
|
|
|
|
|
|