Introduction:
Supernumerary teeth are developmental disturbances occurring during odontogenesis resulting in the formation of teeth in excess of the normal series. They occur both in the deciduous and in the permanent dentition, but their occurrence is more in permanent dentition. In the primary dentition the incidence is 0.3-0.8% and in the permanent dentition it is 1.5-3.5% with a male to female occurrence ratio of 2:1.[1],[2] Supernumerary teeth may be single, multiple, unilateral or bilateral, erupted or unerupted and in one or both the jaws.[3] Single supernumeraries occur in 76-86% of cases, double supernumeraries occur in 12-23% of cases and multiple supernumeraries in less than 1% of cases.[4],[5],[6],[7]
These teeth can be classified in the following manner. Firstly, according to their location in the dental arch a supernumerary can either be classified as amesiodens, paramolar ordistomolar. Secondly, they can be classified according to their morphological forms as conical, tuberculate, supplemental or an odontome.[8] A mesiodens is a supernumerary located in between the central incisors in the maxilla. A paramolar is one situated bucally or palatally to one of the maxillary molars. A distomolar is situated distal to the third molar.
A conical supernumerary is a small peg shaped (coniform) tooth with a normal root. Tuberculate (multicusped) supernumerary tooth is a short barrel shaped tooth with normal or invaginated crown but rudimentary root. A supplemental tooth refers to a supernumerary tooth of normal size and shape and resembles the normal series(duplication). Most of the supernumerary in the primary dentition are of the supplemental type. In the permanent dentition they are more common in the maxillary lateral incisor region.Odontome is a supernumerary having no regular shape of a tooth but it is usually multiple in nature.
There are many complicationswhich have been associated with supernumeraries,like impaction of adjacent teeth, delayed or ectopic eruption of relevant teeth, crowding, rotation and development of midline diastemaof permanent incisors. There are reports that a supernumerary may erupt into the floor of nasal cavity instead of oral cavity. A supernumerary may give rise to development of dentigerous cyst.[9],[10]
The aim of this report is to document two cases. First an interesting case of four impacted supernumeraries without any associated syndrome and a case of impacted supernumerary tooth resulting in the rotation of permanent left central incisor.
Case Report:
An 11 year old female patient reported to the Department of Pedodontics and Preventive Dentistry, Himachal Dental College, Sundernagar, H.P with the chief complaint of malaligned front teeth. The patient had no significant medical historysuggesting the presence of any syndrome. The dental history did not suggest any trauma to the front teeth as well. Intra-oral examination revealed proclined maxillary permanent left central incisor with diastema in between central incisors (Figure 1). On palpation the supernumerary teeth could neither be
 | Figure 1. Intra Oral Photograph Of Case 1 Radiograph
 |
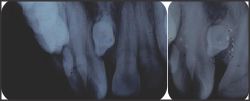
 | Figure 2: Occlusal
|
 | Figure 3: Intraoral Periapical Radiographc
|
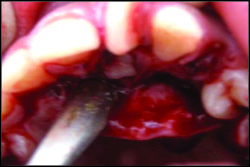
 | Figure 4: Buccal And Palatal Flap Raised
|
 | Figure 5: All Teeth Removed
|
 | Figure 6: Four Supernumerary Removed
|
felt on labial nor on palatal sides of the incisors.The occlusal and intra-oral periapical radiographs revealed the presence of multiple supernumerary teeth in the mid line of maxilla (Figure 2,3).
The treatment plan comprised of surgery followed by the orthodontic intervention. After adequate anaesthesia was obtained, an incision in the alveolar ridge was made. Both buccal and palatal flaps were raised. With the help of an elevator all four supernumerary teeth were removed. The flaps were closed with sutures (Figure 4,5,6,7).
Prior to proceeding for surgical procedures routine blood and urine examinations were carried out and the results were found to be within the normal limit. A course of antibiotics and analgesics were prescribed to prevent any post-operative complications. The patient was advised to maintain a good oral hygiene. After sufficient bone was formed into the surgical wounds, the patient was referred to the department of orthodontics for alignment of teeth.
Case Report:
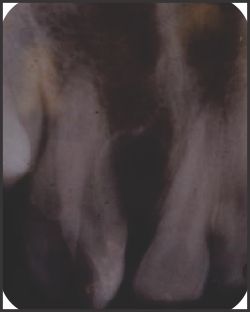
A 12 year old male patient reported with the chief complaint of malalignedfront teeth. Intra oral examination revealed rotated permanent left central incisor (Figure 8).An intra-oral periapicalradiograph as well as occlusal radiograph were taken immediately. Theyrevealed the presence of an impacted supernumerary tooth in relation to the left central incisor (Figure 9).
The anaesthesia was administered. The palatal mucoperiosteal flap was raised from upper right canine to left first premolar. The bone cutting was minimumas the supernumerary was lying just below the mucoperiosteum. With the help of an elevator the supernumerary was removed and the flap was closedafter thorough debridement and cleaning (Figure 10,11). The postoperative instructions and management were same as described before.
After proper healing of the wounds and filling of the bone cavity with new bone, we planned to go for the orthodontic correction of therotated permanent left central incisor (Figure 12,13,14).
Discussion
 | Figure 7: Post-operative Radiograph
|
 | Figure 8: Intra oral photograph
|
 | Figure 9: Occlusal and Intra oral of case 2periapical radiographs
|
 | Figure 10: Supernumerary Tooth Visible
|
 | Figure 11: Post-operative Radiograph On Raising The Palatal Flap
|
 | Figure 12: Fixed Orthodontic Treatment
|
 | Figure 13: Partial Correction Of 21 In Progress
|
 | Figure 14: Correction Done
|
The etiology of supernumerary teeth remains unclear, but several theories have been been suggested. The hyperactivity of the dental lamina is the most accepted cause.[11] According to this theory, remnants of dental lamina are thought to induce development of an extra tooth bud which results in a supernumerary. A second theory is the dichotomy theory, which suggests that the tooth bud is split to create two teeth.[12]The supplemental teeth may explain the presence of this theory.Along with these two theories genetics has also been considered in the development of supernumerary teeth as multiple supernumeraries are associated with various syndromes.
The multiple supernumerary teeth are usually associated withDowns syndrome,Gardners syndrome,Cleidocranial dysplasia, Cleft lip and palate, Orodigito facial dysostosis.[5],[6],[13],[14] The present case reveals the presence of multiple supernumerary teeth in a non syndromic patient. According to Munns, the earlier the offending tooth is removed the better is the prognosis.[15] But there are some controversies regarding the removal of supernumerary teeth in the mixed dentition period. Most of the authors recommend surgical removal of supernumerary tooth as and when half of the root of the adjacent permanent incisors was formed. This is to minimize injury to the developing permanent tooth.The treatment therefore comprised of surgical removal of supernumerary tooth followed by orthodontic intervention.
In the second case the impacted supernumerary tooth resulted in rotation of left permanent central incisor along with presence of crowding.In this case there was lack of space for the accommodation of the rotated left central incisor. The rotation of left central incisor tooth was corrected with fixed appliance therapy. The tooth is now well aligned in the maxillary arch after about 9 months of active treatment (Figure 12,13,14). The retention of rotation cases should be done with fixed appliance and for a long period of time to prevent relapse.
References
1. Mason C, Azam N, Holt RD and Rule DC (2000). A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J OralMaxillofacSurg, 38: 6
2. Sharma A. Familial occurrence of mesiodens: A Case report. J Indian SocPedoPrev Dent 2003;21:2.
3. RajendranR,Sivapathasundram B. Shafer's Textbook of oral pathology,5th ed. Elsevier: New Delhi, India; 2006.
4. Scheiner MA, Sampson WJ. Supernumerary teeth: a review of the literature and four case reports. Aust Dent J .1997; 42:160-165.
5. Rajab LD, HamdanMA.Supernumerary teeth: review of the literature and survey of 152 cases.Int J PaediatrDent 2002;12:244-254.
6. Zhu JF, Marcushamer M, King LD, Henry JR.Supernumerary and congenitally absent teeth:a literature review. J ClinPediatr Dent. 1996;20:87-95.
7. So LLY.Unusual supernumerary teeth.Angle Orthod.1990;60:289-292.
8. Mitchell L(1989). Supernumerary teeth. Dent Update 16:65-69.
9. Hattab FN, YassinOM,Rawashdeh MA. Supernumerary teeth :Report of three cases and review of the literature.J Dent Child 1994;61:382-93.
10. SolaresR.The complications of late diagnosis of anterior supernumerary teeth: Case report. J Dent Child 1990; 57:209-11.
11. Primosch RE. Anterior supernumerary teeth-assessment and surgical intervention in children.Pediatr Dent 1981;3:204-15.
12. Sedano HO, Gorlin RJ. Familial occurrence of mesiodens.OralSurg Oral Med Oral Pathol 1969;27:360-1.
13. Bohn A. Dental anomalies in harelip and cleft palate.ActaOdontol Scand.1963;21:1-114.
14. Kantor ML, Bailey CS, Burkes EJ. Duplication of the premolar dentition.OralSurg Oral Med Oral Pathol. 1988;66: 62-64.
15. Munns D. Unerupted incisors. Br J Orthod. 1981;8:39-42. |