Introduction
The phenomenon of tooth fusion arises through union of two normally separated tooth germs, and depending upon the stage of development of the teeth at the time of union, it may be either complete or incomplete. On some occasions, two independent pulp chambers and root canals can be seen. Fusion occurs during the morphodifferentiation of the dental germs and the outcome depends on the degree of development of the teeth involved.[1] It is also caused by the persistence of the dental lamina between two or more tooth germs, or, by the attempt of a supernumerary tooth to develop from the remnants of the dental lamina after it has divided from a neighboring tooth germ. The union can be at enamel /dentin with common pulp chamber or separate pulp chambers. When it occurs precociously it may be that the two developing teeth unite to form what appears clinically as a single tooth of normal size.[2] However, if it occurs at a more advanced stage of development the outcome is a tooth of double size or a tooth with bifid crown.
In addition to affecting two normal teeth fusion may also occur between normal tooth and a supernumerary tooth such as mesiodens and distomolar. This developmental anomaly is most often confused with gemination. However, a differential diagnosis can be made radiograpically.[3] It is generally accepted that fusion results from the cojoining of two separate pulp canals, while gemination originates when one tooth bud attempts to split into two.[2],[4] In clinical situations, cases of fusion have the appearance of a congenitally missing tooth, while in gemination the number of teeth in the dentition is normal per quadrant, provided the double teeth is counted as one unit.
This paper reports a rare case of fusion of deciduous mandibular incisors along with bilateral fusion in succadeneous permanent teeth.
Case Report
A 3-year-old male child reported to Department of Pedodontics and Preventive Dentistry with a chief complaint of unusually large lower anterior teeth. Intraoral clinical examination revealed that patient was in a deciduous dentition period and the number of teeth present in mandibular arch were less than normal and the teeth (71,72 and 81,82) were fused together [Fig.1]. Periapical radiographic examination revealed the complete fusion of central and lateral incisors with one root and one pulp canal [Fig. 2] on both sides of mandible, along with the bilateral fusion of associated permanent successors of right and left central and lateral incisor which is an unusual dental anomaly. OPG was advised which confirmed this finding [Fig.3]. There was no history of pain or discomfort and incisors were caries free. The hair and skin of the patient appeared normal and no systemic abnormality or congenital disease was noted in the medical history of the patient and her family.
 | Figure 1: Intraoral View Showing Fusion Of Deciduous Incisors.
 |
 | Figure 2: IOPA Showing Complete Fusion With One Root And One Pulp Canal.
|
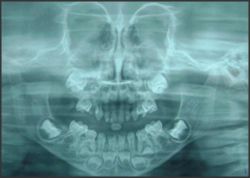 | Figure 3: O.P.G Showing Fused Deciduous And Permanent Incisors.
|
Treatment plan for the patient included follow up till the deciduous fused incisors are shed off and fused permanent incisors erupt. The fused permanent incisors will then be kept under observation for their abnormal morphology and excessive mesiodistal width which can cause problems with spacing, alignment and function.
Discussion
Connated teeth are the consequences of developmental anomalies leading to the eruption of joined elements. According to current definitions, gemination occurs when one tooth bud tries to divide, while fusion occurs if two buds unite.[5]
Fusion is the union of two teeth by dentin and enamel. It has been thought that some forces or pressure produces impact of the developing tooth germs and subsequent union of enamel organ and the dental papilla resulting in union of enamel organ and the dental papilla resulting in fusion of teeth or genetic inheritance can be a possible etiology.[6] If this contact occurs early at least before calcification begins, the two teeth may be completely united to form a single large tooth.
Bilateral mandibular fusion of the primary incisors is a rare event, occurring with a prevalence of less than 0.02%[7]. When all four permanent successors are also bilaterally fused, this event becomes rarer still. Patients with fused incisors have less than a 20 percent chance of having a missing permanent tooth.[8] Epidemiological studies showed that the prevalence of fused teeth was similar for girls and boys and occurred most frequently in the primary dentition.[9]
Four morphological types of fusion were identified by Aguiló L, Gandia JL, Cibrian R, Catala M[10]: type I- bifid crown-single root; type II- large crown-large root; type III- two fused crowns-single root; type IV- two fused crowns-two fused roots. Type I was seen only in the maxilla and types II and III only in the mandible. Type IV was seen mostly in the maxilla. In this case, Type III fusion was observed.
Fused teeth are usually asymptomatic. Teeth with these abnormalities are unaesthetic due to their irregular morphology. They also present a high predilection to caries, periodontal disease and spacing problems. The main periodontal complications in fusion cases occur due to the presence of fissures or grooves in the union between the teeth involved.[2],[3] In a preventive concern, the buccal and lingual vertical grooves of double primary teeth may be pronounced and difficult to clean, and are highly susceptible to caries. The placement of fissure sealants or composite restorations in these grooves should decrease the caries risk.[9]
Several clinical problems in the permanent dentition follow fused primary teeth such as physiological root resorption of fused deciduous teeth being retarded due to greater root mass and increased area of root surface, leading to delayed or ectopic eruption of permanent successors.
A rare case of fusion between maxillary primary central incisors and supplemental teeth occurring bilaterally, accompanied by succedaneous supernumerary teeth has also been cited by Tomizawa M, Shimizu A, Hayashi S, Noda T which involved extraction of the supernumerary teeth for eruption of permanent teeth and their careful monitoring.[11] Porcelain veneers and crowns can enhance the esthetic appearance.
In this case there was complete fusion of deciduous central and lateral incisors on both side of mandible, along with the bilateral fusion of associated permanent successors of right and left central and lateral incisor which is an unusual dental anomaly.
References:
1. Ten Cate AR. Oral Histology: Development, Structure, and Function. St. Louis, MO: Mosby; 1998:81-102.
2. Turell IL, Zmener O. Endodontic therapy in a fused mandibular molar. J Endod 1999; 25: 208-9.
3. Camm HJ, Wood AJ. Gemination, fusion and supernumerary tooth in the primary dentition - report of case. ASDC J Dent Child 1989; 56: 60 -1.
4. Nunes E, de Moraes IG, de Novaes PM, de Sousa SM. Bilateral fusion of mandibular second molars with supernumerary teeth- A case report. Braz Dent J 2002; 13:137-41.
5. Neves AA, Neves ML. Bilateral connation of permanent mandibular incisors: a case report. Int J of Paediatr Dent 2002; 12:61-5.
6. Saxena A, Pandey RK, Kamboj M. Bilateral fusion of permanent mandibular incisors: a case report. J Indian Soc Pedod Prev Dent 2008; 26 Suppl 1:S32-3.
7. Milano M, Seybold SV, McCandless G, Cammarata R. Bilateral fusion of the mandibular primary incisors: report of case. ASDC J Dent Child 1999;66:280-2, 229.
8. Hagman FT. Anomalies of form and number, fused primary teeth, a correlation of the dentitions. ASDC J Dent Child 1988; 55:359-61.
9. Peyrano A, Zmener O. Endodontic management of mandibular lateral incisor fused with supernumerary tooth. Endod Dent Traumatol 1995; 11:196-8.
10. Aguiló L, Gandia JL, Cibrian R, Catala M. Primary double teeth. A retrospective clinical study of their morphological characteristics and associated anomalies. Int J Paediatr Dent 1999; 9:175-83.
11. Tomizawa M, Shimizu A, Hayashi S, Noda T. Bilateral maxillary fused primary incisors accompanied by succedaneous supernumerary teeth: report of a case. Int J Paediatr Dent 2002; 12:223-7. |