Introduction
Endodonticpost graduate programs include a wide gamut of subjects varying from the ones which are daily practiced to the ones which are not often imbibed by the budding endodontists in their daily practice besides their importance.Endodontic Glidepath preparationfalls into the latter category.
According to West(2010),[1] the endodontic Glidepath is a smooth radicular tunnel from canal orifice to physiologic terminus (foraminal constriction). Its minimal size should be a "super loose No. 10" endondontic file. The Glidepath must be discovered if already present in the endodontic anatomy or prepared if it is not present. The Glidepath can be short or long, narrow or wide, essentially straight or curved.
According to Ronald et al (2002)[2] and Peters et al (2003)[3], the risk of instrument fracture can be reduced by performing coronal enlargement of the root canal. Blum et al (2003)[4] suggested that a glide path should be created with small stainless steel hand files to create or verify that within any portion of root canal there will be sufficient space for rotary instrument to follow. In 2004, Berutti et al[5] recommended manual preflaring of the root canal to create a glide path before using NiTi rotary instrumentation. They advocate that the root canal diameter should be atleast one size larger as the tip of the first rotary instrument to be used in that root canal. They also reported that a reduction in torsional stress increased the average lifespan of instrument almost six-fold with a reduced risk of instrument fracture.
The adoption of new treatments, techniques or concepts depends not only on their effectiveness or biological rationale but also on operator's preference for and satisfaction in performing such procedures (Granados et al. 1997).[6] Some clinical procedures are not widely implemented for simple reason that they are too difficult or too inconvenient to perform, even though they have strong biological rationale. Undoubtedly, biological principles of endodontic treatment are violated when rubber dam is not used, yet a majority of practitioners continue to practice in such manner (Whitworth et al 2000,[7] Slaus & Bottenberg 2002).[8] From a public health care point of view, the issue of treatment efficiency and cost is also important because resources in the society are limited in a developing nation as ours. Hence they should be directed to the most effective and the most efficient treatment regimen. Decisions making by clinicians appears to be complex and multidimensional. So a study was planned and conducted to assess certain endodontic practices like preparation of glide path among endodontic postgraduate students in India.
This questionnaire based study aimed at gauging awareness and practice of preparing glide path among endodontic post graduate students throughout the nation.
Materials And Methods
A questionnaire survey was used to tabulate opinions and awareness of the postgraduate endodontic students in India concerning the preparation of the glide path while performing root canal treatment. 320 survey forms were mailed electronically to Post graduate students and 180 were distributed at a national conference. The respond rate was 75% by former and 80% by latter method i.e. a total of 444 filled survey forms were finally evaluated in the study. Questionnaire comprised of 8 questions in all. The questions were framed to cover all the possible aspect concerning the preparation of glide path. (Table 1).
Table 1. Sample Of Glidepath Survey Letter To Endodontists.
1. Do you know what is glide path?
Yes, i always prepare.
Yes, i prepare it occassionally
Yes, but I don't prepare...
I don't have any idea
2. What size hand file do you prefer for your Glidepath(choose one) ?
#10 size
#15 size
#20 size
more than 20
3. Do you use straight manual files or do you precurve them(choose one) ?
Straight
PreCurved
4. Do you "go to length immediately" or do you do "early coronal enlargement" (choose one)?
Immediately if I can.
Early coronal enlargement
5. What is your preferred irrigating solution(choose one) ?
Sodium hypochlorite
EDTA
Viscous irrigators like RC-Prep, Glyde
Combination of above
6. How do you determine your Glidepath length (choose one)?
Apex locator
Radiographically
Tactile
Combination of above
7. Which radiographic technique would you use ?
RVG
Simple radiograph
8. When making the Glidepath, what hand motion do you use (ie, "watch/wind”,"push/pull," or other) ?
Watch-winding
Push-pull
Both
Others
Results
Only 30 % of respondents always prepare a glide path in their practice. Most of them (60%) prepare it occasionally, 20% never prepared it and 10 % did not have any idea of glide path preparation. 55% of respondents precurve the file before inserting into canal whereas 45 % preferred to use it straight. (Figure 1 and Table 2), (Figure 2 and 3).
Most of post graduate students preferred prefer "watch/wind." (Figure 4)
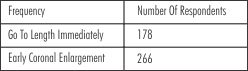 | Table 2. Go to Length Immediately or Early Coronal Enlargement
 |
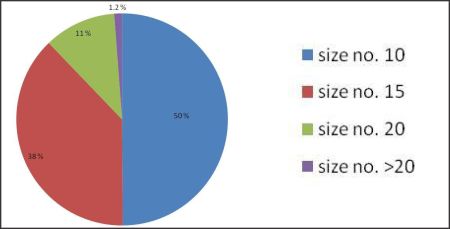 | Figure 1. Hand File Size Preference.
|
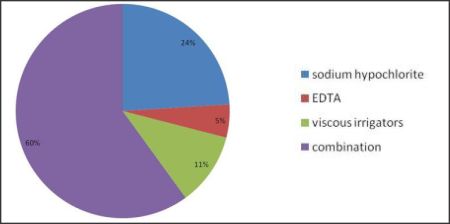 | Figure 2. Irrigation Solution Preference.
|
 | Figure 3- determination of glide path length
|
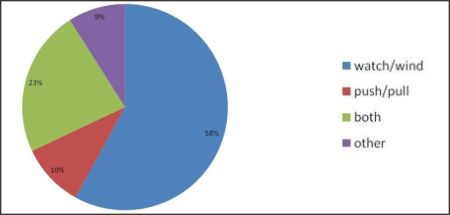 | Figure 4. Hand Motion Preference.
|
Discussion
Many clinicians instrument the curve in the canal exclusively by hand and only use rotaries for the straight part of the canal. There are also some clinicians who use hand instruments greater than a No. 10 to make a glide path (50 % of respondents use greater than a No. 10 file to make a glide path ). Neither of these approaches is advisable because hand instruments greater than No. 10 in the canal may cause an iatrogenic event. Even if a No. 15 hand file passes through a severely curved canal initially, very often it will not be able to negotiate the curve a second time. The only hand instrument that should be used in a severely curved canal is a No. 8 or a No. 10 reamer, which will follow the curve without any need to pre-bend (50 % of respondents use No. 10 file for preparing glide path according to this survey). Just like a tooth with a severe curve must be loosened with either proximators, luxators, elevators, or periotomes before the extraction forceps are employed so that the root does not fracture during the extraction process, so too a well-defined glide path must be made to prepare the curved canal for instrumentation and shaping. Melvyn Segal in 2008[9] has found through experimenting on extracted teeth with curved canals that hand instruments above No. 10 can easily create a ledge or transport or zip the apex. Often, a zip or transportation may not even be apparent on a radiograph. The clinician will believe that he or she performed the perfect root canal on a curved root, when in reality the canal was transported or zipped.
When preparing a straight canal, any system will work. But when it comes to a severely curved canal, the curve has to be well-prepared by precurving the instrument (55 % of post graduate students precurve their instruments according to this survey) before using any of the systems to prevent an iatrogenic event.
60 % of post graduate students prefer to do early coronal enlargement before going to apex. Slightly more post graduate students prefer early coronal enlargement, primarily due to the presence of restrictive dentin which restricts finesse and mastery of the first Glidepath file.
Most of the post graduate students prefer to use combination of NaOCl, EDTA and viscous chelators for preparing glide path. Sodium hypochlorite and a viscous chelator (or a combination of the 2) enable digestion of necrotic pulp and the ability to emulsify vital pulp.
Working length determination is one of the most critical steps in endodontics, as it facilitates biomechanical preparation and obturation of the root canal system. Failure to accurately determine the length of the root canal often results in apical perforation, over instrumentation and other mishaps which leads to root canal failure.
A majority of the respondents (34 %) were using the radiographs to determine the working length. This method has inherent inaccuracies, as the apical foramen may not be detectable on radiographs. Electronic apex locator has the advantage of being able to locate the apical foramen. Nevertheless, electronic apex locator is not the substitute for radiographs since the latter provide valuable information about root canal morphology as well. So combination of these methods should be preferred. 40 % of respondents preferred to use combination of radiograph and electronic apex locator. The combination of apex locator and radiographic terminus, is the clinician's choice. Canal length accuracy is excellent when both methods of length determination validate each other. The important thing to remember is that the length is dynamic and becomes shorter, especially in the early stages of rotary shaping, due to canal shortening.
In 2006, West[10] recommended using a K-file with an initial watch winding motion to remove restricted dentin in very narrow canals, followed by a vertical in and out motion with a 1mm amplitude as the dentin wall wears away and the file advances apically. Most endodontists prefer "watch/wind." Only 9% chose "other." These motions make endodontic files efficient when the dentist learns how, when, and why to use what motion. Glidepath demands that the dentist "thinks" and is "deeply present," resisting all distractions.
Conclusion
Without the endodontic Glidepath, the rationale of endodontics cannot be achieved. A nonsurgical seal requires first the creation of a radicular path that can be cleaned of viable and nonviable bacteria, vital and nonvital pulp tissue, biofilm, and smear layer; then shaped to a continuously tapering funnel that can be predictably and easily obturated. Moreover, Glidepath is necessary for quality control. Sustainable excellent endodontic obturations are not possible without it.
The preparation of glide path is important in endodontics so the professional bodies in endodontics should embark on training programs, seminars and workshops aimed at improving the knowledge and skills of the endodontists. Appropriately structured continuing education courses and journals may be able to meet the demands and needs of endodontists in India.
References
1. West J. The Endodontic Glidepath: Secrets to rotary success. Dentistry Today 2010; 29(9): 90-9343.
2. Roland DD, Andelin WE, Browning DF, Hsu GR, Torabinejad M. The effect of preflaring on the rates of separation for 0.04 taper nickel-titanium rotary intruments. J Endod 2002; 28(7): 543-545
3. Peters OA, Peters CI, Schonenberg K, Barbakow F. ProTaper rotary root canal preparation: assessment of torque and force in relation to canal anatomy. Int Endod J 2003; 36: 93-99.
4. Blum JY, Machtou P, Ruddle CJ, Micallef JP. The analysis of mechanical preparations in extracted teeth using protaper rotary instruments: value of the safety quotient. J Endod 2003; 29: 567-575
5. Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of manual preflaring and torque on the failure rate of Protaper instruments. J Endod 2004; 30: 228-30
6. Granados A, Jonsson E, Banta HD et al. EUR-ASSESS Project Subgroup Report on dissemination and impact. International Journal of Technology Assessment in Health Care 1997; 13: 220-86.
7. Whitworth JM, Seccombe GV, Shoker K, Steele JG. Use of rubber dam and irrigant selection in UK general dental practice. International Endodontic Journal 2000; 33: 435-41.
8. Slaus G, Bottenberg P. A survey of endodontic practice amongst Flemish dentists. International Endodontic Journal 2002; 35: 759-67.
9. Melvyn Segal. Managing Curved Canals: the Straight-Away and Super Glide Path Technique. Inside Dentistry April 2008, Volume 4, Issue 4
10. West J. Endodontic update . J Esthet Restor Dent. 2006;18:280-300. |