Introduction:
Cleaning and shaping of the root canal system is one of the important phases of root canal treatment procedure.[1] It includes mechanical debridement, creation of space for medicament delivery, and forming optimized canal geometries for adequate obturation.[2] In the course of cleaning and shaping the root canal system, the clinician needs to determine three clinical parameters. These are length of the canal, the taper of the preparation and the horizontal dimension of the preparation at its most apical extent also called the initial apical file size.[3]
For cleaning and shaping of a root canal, most clinicians start by selecting a first file that they believe fits at the apex and enlarge in relation to that file diameter.[4] It has been suggested that the amount of apical enlargement to be achieved during shaping of the canal should be three file sizes greater than the first file that fits at the apex.[3] Determination of the first file that binds at the working length is based on the tactile sensation of the clinician.[5] However, various factors such as, cervical constriction, canal length, canal taper, canal curvature, canal content, canal wall irregularities and the instrument used for determining the initial working width, may influence the tactile discrimination.[3] Studies have shown that the enlargement of the coronal and middle third of the root canal allows a more accurate assessment of the initial apical canal diameter.[5]
Cervical preflaring can be performed by different instruments. While Gates-Glidden drills have been used for pre-enlarging the coronal two thirds of the root canals since ages; contemporary nickel titanium (NiTi) rotary systems have specially designed files for cervical preflaring. Their characteristic instrument design influences the coronal preflaring of the canal.[5], [6] ProFile instruments were one of the first NiTi instruments,[7] while K3 is one of the newer rotary NiTi instrument systems hence we are taking these systems[8].
This in vitro study is an attempt to evaluate the influence of cervical preflaring of root canals performed with Gates-Glidden drills, ProFile orifice openers and K3 body shaper files, on the accurate determination of initial apical canal diameter using stereomicroscope.
Material and Methods:
Selection and preparation of samples
Sixty recently extracted human maxillary permanent molars with relatively straight, non-fused, divergent roots were used in this study using all universal aseptic precautions. Conventional endodontic access cavities were prepared and the teeth were checked for patency and for the presence of a single root canal per root. The selected teeth were stored in normal saline at room temperature until further use.
Procedure:
The root canal of each root was explored using a size 10 K-file until the apical foramen was reached and the tip of the file was visible. The actual canal length was determined and working length was established by deducting 1 mm. Cusp tips were used as reference points because the study is In-vitro. Both the working length and the reference point of each individual canal were recorded. All the canals in each tooth were included in the study. A total of 180 canals were eventually utilized. Each tooth was stored in an individually labelled, capped plastic vial containing normal saline.
Sizing of Canals.
Each canal in all the selected teeth was sized with stainless steel K-files in random order. Handles of files were painted black in order to avoid the identification. Files were inserted passively into the canal with a light 'watch-winding' action and care was taken to avoid any force during sizing. File size was increased until binding sensation was felt at the working length. Measurement was undertaken starting from ISO size 10 and the biggest file size that reached the correct working length was recorded. The size of file was recorded as first file fitting at the apex (FFFA) before flaring (FFFAb). After this, samples were divided into four experimental groups of fifteen teeth each.
In Group Ino cervical preflaring of root canals was performed, while in group II, group III and group IV cervical preflaring was achieved by using experimental instruments. The procedure of cervical flaring for each group was as follows:
Group I- Without cervical preflaring
This group received the initial apical instrument without previous preflaring of the root canal.
Group II- Cervical preflaring with Gates-Glidden drills
In this group root canals were preflared with Gates-Glidden drills using endodontic electronic torque control motor X- SMART as per manufacturer's instructions.[6]Flaring began with Gates-Glidden #4 and continued with a Gates-Glidden #3, 2, 1 extending the shaping further apically till resistance felt.Canal patency was checked and irrigation continued.
Group III- Cervical preflaring with ProFile orifice openers
Cervical flaring was done with ProFile instruments using a crown-down approach according to manufacturer's instructions.[7] Flaring began with ProFile orifice opener 3 (#40, 0.06 taper),and continued with aProFile orifice opener 2 (#30, 0.06 taper), ProFile orifice opener 1(#20, 0.06 taper) extending the shaping further apically till resistance felt.
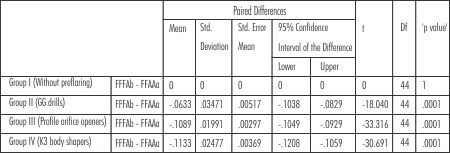 | Table 1
 |
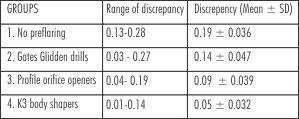 | Table 2
|
 | Figure 1
|
Group IV- Cervical preflaring with K3 body shaper files
In this group cervicalflaring was done with the K3 enhanced-tapered body shapers using a crown-down approach as per manufacturer's instructions.[8] Flaring began with size 25(0.12 taper) taper orifice shaper and continued with a successively smaller tapered body shapers size 25 (0.10 taper) and 25 (0.08 taper) until the light resistance was felt. Thus, each smaller tapered file advanced further apically ensuring a crown down sequence.
During the preflaring of canals in group II, group III and group IV, 15% EDTA gel was used as a lubricant with each instrument. After each instrument use, canal was irrigated with 2 ml of 3% sodium hypochlorite (Vishal Dentocare Pvt. Ltd.) using a 27 gauge needle-syringe then recapitulated with a #10 file and re-irrigated.
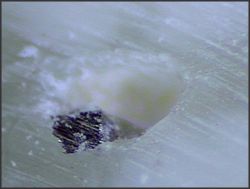
Following this again sizing of each canal was done as described above. Measurement was undertaken starting from ISO size 10 and the biggest file size that reached the correct working length was recorded. This file was recorded as first file fitting at apex after flaring (FFFAa). The file corresponding to the initial apical file (IAF) after preflaring i.e. FFFAa was fixed into the canal at the working length (WL) with cyanoacrylate adhesive. After this, roots of each sample were sectioned transversely 1 mm from the apex using diamond disc. Sectioned apical region was then observed under stereomicroscope (Olympus SZ 4045) at 30 X magnification. Root canal and file maximum diameters were measured directly using a calibrated ocular scale for each sample.
The differences between these measurements were submitted to statistical analysis. A multiple comparison, one variable test (ANOVA) with post-hoc tukey's testwas performed to examine the effect of the four different preflaring techniques on the diameter differences found between root canals and binding instruments. Comparison of the first file that fits to the apex in each canal before and after flaring was performed by the Student- t- test. Mean values and standard deviations were calculated using a paired- t- test and ANOVA. Statistical analysis was performed at the 0.05 level of significance.
Results:
A paired t-test of intragroup values indicated a significant difference (p, 0.001) of file size before and the after flaring for all early flaring groups (Table no. 1).
FFFA- First file fitting at apex
FFFAb- First file fitting at apex before preflaring
FFFAa- First file fitting at apex after preflaring
The increase in mean apical file diameter was approximately one file size for group II, while it was two file sizes for group III and group IV.
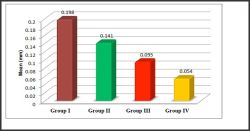
Discrepancies measured between canal diameter at working length and FFFAa with different preflaring techniques by using stereomicroscope at 30 X magnification are presented in (Table 2) and (Fig.1).
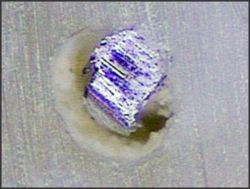
The major discrepancy was found in group I, where no cervical preflaring was performed (0.19 mm average, Fig. 2). The K3 body shaper files produced the smallest differences between anatomical diameter and first file to bind (0.05 mm average, Fig. 3). ProFile orifice openers were found second and Gates Glidden drills third best with statistically significant results (0.09 mm, Fig. 4 and 0.14 mm, Fig. 5 respectively).
Discussion:
The biomechanical preparation of the apical region is an essential and critical operative step of endodontic therapy.[9] Many in vitro studies have recorded the scales and average sizes of root canals, but there have been few clinical attempts to determine the working width. The horizontal dimension of the root canal system is not only more complicated than the vertical dimension (root canal length or working length) but also more difficult to investigate because the horizontal dimension varies greatly at each vertical level of the canal. [3]
Apical access by cervical preflaring has been increasingly investigated , the procedure aims to remove cervical interferences from the root canal entrances which represent an obstacle to free access of endodontic instruments to the apical portion of the root canals, which in turn enhances canal shaping at the apical third.[10] Preflaring can be done with either manual or rotary instruments. Rotary flaring is more rapid than hand and reduces the treatment time; in addition flare, smoothness and uniformity of the canal preparation are also better. Early flaring, regardless of the method used, removes these contacts, opens the space and reduces file contact, thus a file progresses more easily toward the apex and comes to a stop only when the diameter of the canal begins to apply pressure against the instrument. This better sense of apical diameter provides information that should result in better biomechanical preparation.[4]
 | Figure 2
|
 | Figure 3
|
 | Figure 4
|
 | Figure 5
|
The findings of the present study showed the increase in mean apical file diameter after preflaring was approximately one file size for group II, whereas it was two file sizes for group III and group IV. This can be attributed to differences in design features of the instruments used in terms of their ISO size and taper resulting in different amount of removal of cervical interferences in each group.[11]
There was a statistically significant difference (p <0.05) amongst groups, concerning the discrepancy between anatomical diameter at working length and the first file to bind in the canal. From all the rotary instruments evaluated in this study (Gates-Glidden drills, ProFile orifice openers and K3 body shaper files), canals preflared with K3 body shaper files (Group IV) presented the lowest discrepancy values between the file size and anatomical diameter whichcan be attributed to modified design ofK3 body shapers which include enhanced taper which allow complete removal of cervical interferences.[8], [10], [12]
Groups preflared with ProFile orifice openers (Group III) and Gates Glidden drills (Group II) were found second and third best respectively with statistically significant results. The performance of ProFile orifice openers is due to their U-file radial-landed flute design that provides optimal cutting efficiency and allows for greater removal of interferences in the cervical third.[7], [13]
The Gates Glidden drills straightened the coronal two- thirds of the root canals in an attempt to reduce binding in the coronal region which provided direct access to both the cervical and middle thirds of root canals, reducing the contact area of the instrument in these regions. When used adequately GG instruments are inexpensive, safe and clinically beneficial tools, nevertheless, these instruments did not allow for accurate determination of the initial apical file. [5], [9], [12]
Conclusion:
The findings of our study clearly suggest that cervical preflaring of canals is necessary for the better cleaning and shaping of the root canal as it facilitates more accurate determination of initial apical file size. The preflaring was best with K3 body shaper files as it lead to minimal discrepancy between initial apical file size diameter and canal diameter at working length.
References:
1. Nagy CD, Bartha K, Bernath M, Verdes E andSzabo J. A comparative study of seven instruments in shaping the root canal in vitro.Int Endod J 1997; 30: 124-32.
2. Ove PA.Current challenges and concepts in the preparation of root canal systems: A Review.J Endod 2004; 30:559-567.
3. Jou YT, Karabucak B, Levin J,Liu D. Endodontic working width: current concepts and techniques. Dent Clin North Am 2004; 48:69-85.
4. Contreras MAL, Zinman EH and Kaplan SG. Comparison of the first file that fits at the apex, before and after early flaring. J Endod 2001; 27:113-116.
5. Pecora JD, Capelli A, Guerisoli DMZ. Influence of cervical preflaring on apical file size determination.Int Endod J 2005; 38: 430-435.
6. Peter O and Peters C.Cleaning and shaping of root canal system. Cohen inPathways of the pulp. Ninth edition Mosby, Inc. 179-218.
7. Hsu YY, Kim S. The ProFile system. Dent Clin North Am 2004; 48:323- 35.
8. Mounce RE.The K3 rotary nickel-titanium file system. Dent Clin North Am 2004; 48: 137-157.
9. Schmitz MS, Santos R, Capelli A. Influence of cervical preflaring on determination of apical file size in mandibular molars: SEM analysis. Braz Dent J2008; 19: 245-251.
10. Ibelli GS, Barroso JM, Capelli A.Influence of cervical preflaring on apical file size determination in maxillary lateral incisors.Braz Dent J 2007; 18: 102-106.
11. Tennert C, Herbert J, Altenburger MJ, Wrbas KT.The effect of cervical preflaring using different rotary nickel-titanium systems on the accuracy of apical file size determination.J Endod 2010; 36: 1669-72.
12. Vanni JR, Santos R, Limongi O. Influence of cervical preflaring on determination of apical file size in maxillary molars: SEM analysis. Braz Dent J2005; 16: 181-186.
13. Tan BT and Messer HH.The effect of instrument type and preflaring on apical file size determination. Int Endod J 2002; 35: 752-758. |